商品详情
返回产品目录
商品包装及说明书因厂家更换频繁,如有不符以实物为主
图卡替尼片
国际零售参考价:¥**/盒
-
温馨提醒:本说明书仅供参考,最新的说明书详见药品附带的说明书。
1适应症和用途
TUKYSA与曲妥珠单抗和卡培他滨联用,可用于治疗晚期不可切除或转移性HER2阳性乳腺癌的成年患者,包括脑转移患者,这些患者已在转移环境中接受了一种或多种先前的基于抗HER2的治疗方案。
2剂量和给药
2.1推荐剂量
TUKYSA的推荐剂量为300 mg,每天口服两次,与曲妥珠单抗和卡培他滨合用,直至疾病进展或出现不可接受的毒性[见临床研究(14) ]。
建议患者吞咽TUKYSA片剂整个吞咽,吞咽前不要咀嚼,压碎或分裂。劝告患者不要服用片剂破裂,破裂或不完整的片剂。
劝告患者每天间隔大约12个小时服用TUKYSA,每天或不加餐。
如果患者呕吐或错过了一定剂量的TUKYSA,请指示患者在其通常的计划时间服用下一剂。
当与TUKYSA联合使用时,卡培他滨的推荐剂量为1000 mg / m 2,每天两次,饭后30分钟内服用。TUKYSA和卡培他滨可以同时服用。有关其他信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
2.2不良反应的剂量修改
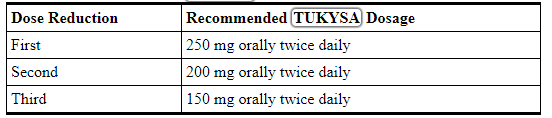
表1 和表 2提供了建议的TUKYSA减少剂量和不良反应剂量的调整方法。有关这些药物剂量调整的信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
表1:不良反应的推荐TUKYSA剂量减少
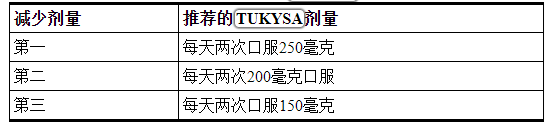
无法每天两次口服150 mg的患者,永久停用TUKYSA。
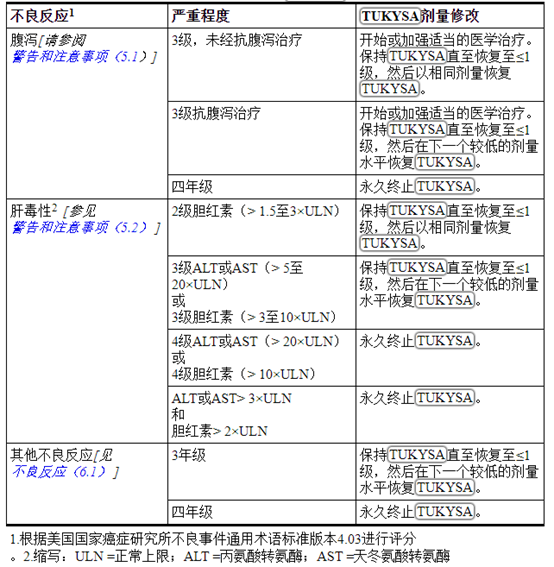
表2:不良反应的推荐TUKYSA剂量修改
2.3严重肝功能不全的剂量调整
对于患有严重肝功能不全(Child-Pugh C)的患者,建议每天两次口服减量至200 mg [ 参见《特定人群的使用》(8.7),《临床药理学》(12.3) ]。
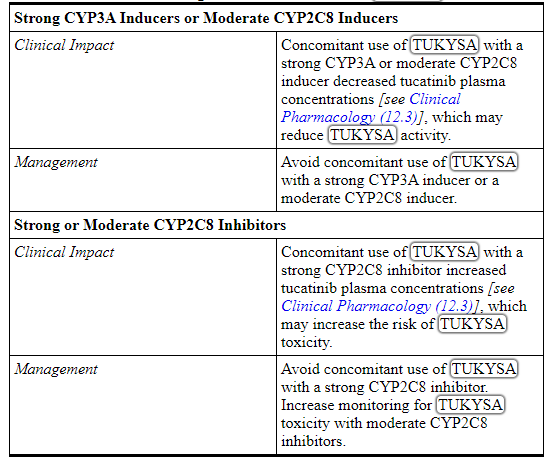
2.4与强效CYP2C8抑制剂同时使用的剂量修改
避免与TUKYSA并用强CYP2C8抑制剂。如果不能避免与强效CYP2C8抑制剂同时使用,建议将口服剂量减低至100 mg,每日两次。终止强效CYP2C8抑制剂的3个消除半衰期后,恢复开始使用抑制剂前的TUKYSA剂量[见药物相互作用(7.2),临床药理学(12.3) ]。
3剂型和强度
平板电脑:
- 50毫克:圆形,黄色,薄膜包衣,在一侧凹陷有“ TUC”,在另一侧凹陷有“ 50”。
- 150毫克:椭圆形,黄色,薄膜包衣,在一侧凹有“ TUC”,在另一侧凹有“ 150”。
4禁忌症
没有。
5警告和注意事项
5.1腹泻
TUKYSA可引起严重的腹泻,包括脱水,低血压,急性肾损伤和死亡[见不良反应(6.1) ]。在HER2CLIMB中,接受TUKYSA的患者中有81%经历了腹泻,其中12%的3级腹泻和0.5%的4级腹泻。两名发生4级腹泻的患者随后均死亡,腹泻是导致死亡的原因。第一次腹泻发作的中位时间为12天,解决腹泻的中位时间为8天。腹泻导致6%的患者减少TUKYSA的剂量,导致 1%的患者停用TUKYSA。HER2CLIMB不需要预防性使用止泻药。
如果出现腹泻,请按照临床指示进行腹泻治疗。根据临床指示执行诊断测试,以排除其他腹泻原因。根据腹泻的严重程度,中断剂量,然后降低剂量或永久停用TUKYSA [ 参见剂量和用法(2.2) ]。
5.2肝毒性
TUKYSA可引起严重的肝毒性[见不良反应(6.1) ]。在HER2CLIMB中,接受TUKYSA的患者中8%的ALT增加> 5×ULN,6%的AST增加> 5×ULN,1.5%的胆红素增加> 3×ULN(≥3级)。肝毒性导致8%的患者减少TUKYSA剂量,而1.5%的患者停用TUKYSA。
在开始TUKYSA之前,应在治疗期间每3周监测一次ALT,AST和胆红素,并根据临床情况进行监测。根据肝毒性的严重程度,中断剂量,然后降低剂量或永久停用TUKYSA [请参阅剂量和给药方法(2.2) ]。
5.3胚胎-胎儿毒性
根据动物研究的结果及其作用机理,TUKYSA对孕妇给药可引起胎儿伤害。在动物生殖研究中,在器官形成过程中向怀孕的大鼠和兔子服用妥卡替尼会导致胚胎致死率,降低的胎儿体重和胎儿异常,而孕产妇的暴露量大于或等于推荐剂量下人类暴露量(AUC)的1.3倍。
建议孕妇和具有生殖潜力的女性对胎儿的潜在危险。劝告有生殖潜力的女性在接受TUKYSA治疗期间以及最后一次给药后至少1周内使用有效的避孕方法。建议男性患者繁殖潜力与治疗过程中使用的有效避孕的女性伴侣TUKYSA和最后一次给药后至少1周[见特殊人群中使用(8.1,8.3)]。
TUKYSA与曲妥珠单抗和卡培他滨联合使用。有关妊娠和避孕的信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
6不良反应
标签上其他地方描述了以下临床上显着的不良反应:
- 腹泻[请参阅警告和注意事项(5.1) ]
- 肝毒性[见警告和注意事项(5.2)]
6.1临床试验经验
由于临床试验是在广泛不同的条件下进行的,因此不能将在某种药物的临床试验中观察到的不良反应率直接与另一种药物的临床试验中观察到的不良反应率进行比较,并且可能无法反映实际中观察到的不良反应率。
HER2阳性转移性乳腺癌
HER2CLIMB
在HER2CLIMB中评估了TUKYSA联合曲妥珠单抗和卡培他滨的安全性[参见临床研究(14) ]。 患者接受每日两次TUKYSA 300 mg加曲妥珠单抗和卡培他滨(n = 404)或安慰剂加曲妥珠单抗和卡培他滨(n = 197)。TUKYSA组的中位治疗时间为5.8个月(范围:3天,2.9年)。
接受TUKYSA治疗的患者中有26%发生了严重的不良反应。≥2%接受TUKYSA治疗的患者的严重不良反应为腹泻(4%),呕吐(2.5%),恶心(2%),腹痛(2%)和癫痫发作(2%)。接受TUKYSA治疗的患者中有2%发生致命的不良反应,包括猝死,败血症,脱水和心源性休克。
接受TUKYSA治疗的患者中有6%发生不良反应,导致治疗中断。导致≥1%的患者停用TUKYSA的不良反应为肝毒性(1.5%)和腹泻(1%)。
接受TUKYSA治疗的患者中有21%发生不良反应,导致剂量降低。≥2%的患者导致TUKYSA剂量降低的不良反应为肝毒性(8%)和腹泻(6%)。
接受TUKYSA(≥20%)的患者最常见的不良反应是腹泻,掌- 红肿,恶心,疲劳,肝毒性,呕吐,口腔炎,食欲下降,腹痛,头痛,贫血和皮疹。
表3总结了HER2CLIMB中的不良反应。
表3:接受HER2CLIMB接受TUKYSA治疗的患者的不良反应(≥10%),与安慰剂相比,两组之间的差异≥5%(所有级别)

表4:接受TUKYSA且与HER2CLIMB安慰剂相比≥5%差异的患者的基线实验室恶化(≥20%)
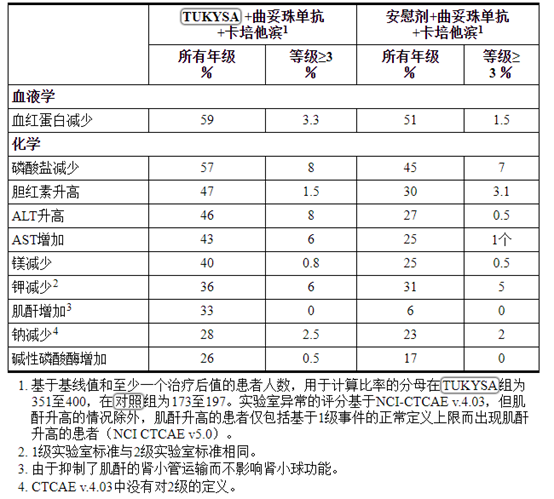
肌酐增加
在用TUKYSA治疗的前21天内,血清肌酐的平均增加为32%。血清肌酐的增加在整个治疗过程中持续存在,并且在治疗完成后是可逆的。如果观察到血清肌酐持续升高,请考虑使用其他肾功能标志物[见临床药理学(12.3) ]。
7药物相互作用
7.1其他药物对TUKYSA的影响
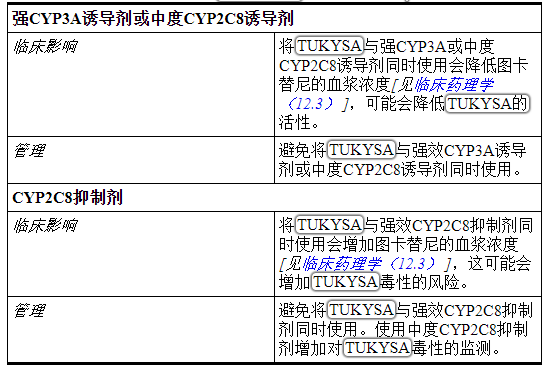
表5总结了其他药物对TUKYSA的作用。
表5:影响TUKYSA的药物相互作用
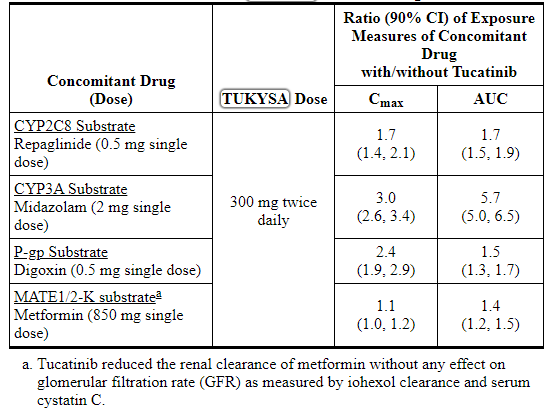
7.2 TUKYSA对其他药物的影响
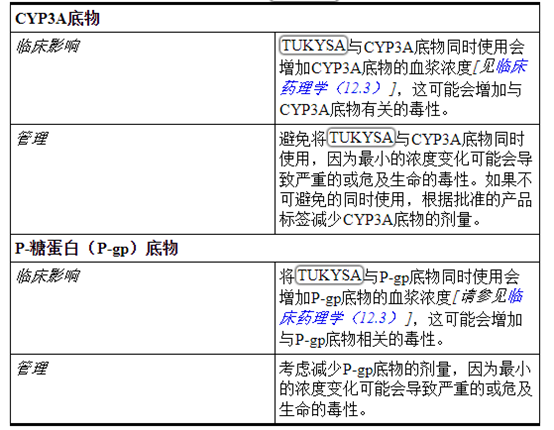
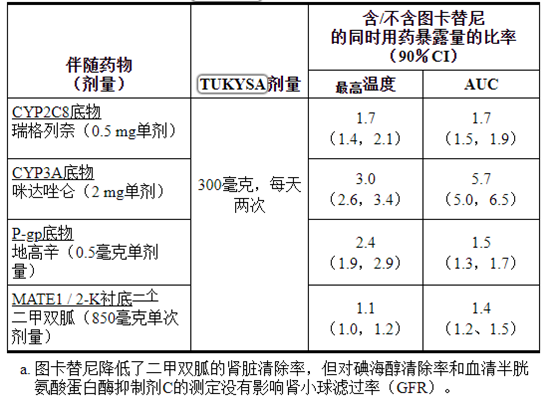
表6总结了TUKYSA对其他药物的作用。
表6:影响其他药物的TUKYSA药物相互作用
8在特定人群中的使用
8.1怀孕
风险摘要
TUKYSA与曲妥珠单抗和卡培他滨联合使用。有关妊娠信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
根据动物中的发现及其作用机理,TUKYSA对孕妇给药可引起胎儿伤害[见临床药理学(12.1) ]。目前尚无有关孕妇使用TUKYSA的人类数据来告知与药物相关的风险。在动物生殖研究中,在器官形成过程中向怀孕的大鼠和家兔施用图卡替尼可导致胚胎-胎儿死亡率,降低的胎儿体重和胎儿异常(孕产妇暴露>推荐剂量下人暴露(AUC)的1.3倍)(参见数据)。建议孕妇和女性生殖潜力对胎儿的潜在危险。
对于所指示的人群,主要出生缺陷和流产的背景风险尚不清楚。在美国普通人群中,临床公认的怀孕中主要先天缺陷和流产的估计背景风险分别为2%-4%和15%-20%。
数据
动物资料
在先期胚胎-胎儿发育研究中,怀孕的大鼠和兔子在器官发生期间接受了最大剂量为150 mg / kg / day的图卡替尼口服剂量。
在大鼠中,图卡替尼的口服剂量≥90 mg / kg / day会导致母体毒性(体重减轻,体重增加减少,食物消耗少)。胎儿影响包括≥90 mg / kg /天的活胎儿数量减少,胎儿体重减少和胎儿异常(骨骼变异增加,骨化不完全)(约为基于AUC推荐剂量的人暴露量的3.5倍)。
在兔子中,口服≥90mg / kg /天的剂量的图卡替尼可导致吸收增加,活胎儿的百分比降低以及骨骼,内脏和外部畸形,这是基于AUC的推荐剂量下人暴露量的1.3倍)。胎儿异常包括头部呈圆顶状,大脑扩张,额骨和顶骨骨化不完全以及顶骨上有一个洞。
8.2哺乳
风险摘要
TUKYSA与曲妥珠单抗和卡培他滨联合使用。有关泌乳信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
目前尚无关于人或动物奶中曲妥替尼或其代谢物的存在或其对母乳喂养的孩子或产奶量的影响的数据。由于母乳喂养的孩子可能会出现严重的不良反应,因此建议女性在使用TUKYSA治疗期间以及最后一次给药后至少1周内不要母乳喂养。
8.3生殖潜力的雌雄
当给孕妇服用时,TUKYSA可能会造成胎儿伤害[见在特定人群中使用(8.1) ]。TUKYSA与曲妥珠单抗和卡培他滨联合使用。有关避孕和不育的信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
验孕
在开始使用TUKYSA治疗之前,请验证具有生殖潜力的女性的怀孕状况。
避孕
女性
劝告有生殖潜力的女性在接受TUKYSA治疗期间以及最后一次给药后至少1周内使用有效的避孕方法。
雄性
建议具有生殖潜能的女性伴侣的男性患者在使用TUKYSA治疗期间以及最后一次给药后至少1周内使用有效的避孕方法。
不孕症
根据动物研究的结果,TUKYSA可能会损害男性和女性的生育能力[请参见非临床毒理学(13.1) ]。
8.4小儿使用
尚未确定TUKYSA在儿科患者中的安全性和有效性。
8.5老年用途
在HER2CLIMB中,接受TUKYSA的 82例患者≥65岁,其中8例≥75岁。≥65岁的患者接受TUKYSA者的严重不良反应发生率为34%,低于65岁的患者为24%。接受TUKYSA和65岁以上患者中最常见的严重不良反应是腹泻(9%),呕吐(6%)和恶心(5%)。在65岁以上的患者中,与年轻患者相比,TUKYSA的有效性没有观察到总体差异。≥75岁的患者很少,无法评估疗效或安全性的差异。
8.6肾功能不全
不推荐将TUKYSA与卡培他滨和曲妥珠单抗联合用于严重肾功能不全的患者(根据Cockcroft-Gault方程估算,CLcr <30 mL / min),因为卡培他滨是严重肾功能不全的患者的禁忌。有关严重肾功能不全的其他信息,请参阅卡培他滨的完整处方信息。
对于轻度或中度肾功能不全(肌酐清除率[CLcr] 30至89 mL / min)的患者,不建议调整剂量。
8.7肝功能不全
严重肝功能不全(Child-Pugh C)患者的图卡替尼暴露量增加。减少重度(Child-Pugh C)肝功能不全患者的TUKYSA剂量[请参阅剂量和用法(2.3),临床药理学(12.3) ]。
轻度(Child-Pugh A)或中度(Child-Pugh B)肝功能不全的患者无需调整TUKYSA的剂量。
11说明
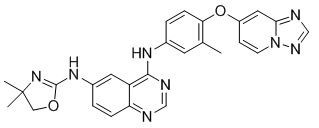
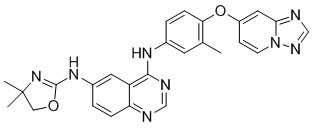
图卡替尼是一种激酶抑制剂。化学名称为(N4-(4-([[1,2,4]三唑并[1,5-a]吡啶-7-酰氧基)-3-甲基苯基)-N6-(4,4-二甲基-4,5 -二氢恶唑-2-基)喹唑啉-4,6-二胺,分子式为C 26 H 24 N 8 O 2,分子量为480.52 g / mol,化学结构如下:
TUKYSA(图卡替尼)以50毫克和150毫克薄膜包衣片剂的形式口服使用,并含有以下非活性成分:
片剂核心:共聚维酮,交聚维酮,氯化钠,氯化钾,碳酸氢钠,胶体二氧化硅,硬脂酸镁和微晶纤维素。
涂层:黄色漆膜:聚乙烯醇,二氧化钛,聚乙二醇/聚乙二醇,滑石粉和未辐照的黄色氧化铁。
每片TUKYSA 50 mg片剂含有10.10 mg(0.258 mEq)钾和9.21 mg(0.401 mEq)钠。
每片TUKYSA 150 mg片剂含有30.29 mg(0.775 mEq)钾和27.64 mg(1.202 mEq)钠。
12临床药理学
12.1行动机制
图卡替尼是HER2的酪氨酸激酶抑制剂。在体外,图卡替尼抑制HER2和HER3的磷酸化,从而抑制下游MAPK和AKT信号传导以及细胞增殖,并在表达HER2的肿瘤细胞中显示出抗肿瘤活性。在体内,图卡替尼抑制表达HER2的肿瘤的生长。图卡替尼和曲妥珠单抗的组合与单独使用任何一种药物相比,在体外和体内均显示出增加的抗肿瘤活性。
12.2药效学
暴露反应关系
图卡替尼的暴露-反应关系和药效学反应的时间过程尚未完全表征。
心脏电生理学
每天两次口服300 mg推荐剂量的TUKYSA治疗后,未检测到QTc的大幅度平均增加(即> 20 ms)。
12.3药代动力学
图卡替尼AUC 0-INF和C max在50 mg至300 mg(批准的推荐剂量的0.17至1倍)的剂量范围内成比例增加。图卡替尼在每天两次给予TUKYSA 300 mg连续14天后,AUC的累积量是1.7倍,C max的累积量是1.5倍。达到稳定状态的时间约为4天。
吸收性
图卡替尼血药浓度达到峰值的中位时间约为2小时(范围为1至4小时)。
食物的影响
在高脂餐后(约58%的脂肪,26%的碳水化合物和16%的蛋白质)对11位受试者施用单次口服剂量的TUKYSA后,平均AUC 0-INF增加1.5倍,T max改变从1.5小时到4小时,并且C max不变。食物对图卡替尼药代动力学的影响在临床上没有意义。
分配
图卡替尼分布的几何平均(CV%)表观体积约为1670 L(66%)。在临床相关浓度下血浆蛋白结合率为97.1%。
消除
图卡替尼的几何平均(CV%)半衰期约为8.5(21%)小时,表观清除率为148 L / h(55%)。
代谢
Tucatinib主要经由CYP2C8代谢,而经由CYP3A代谢的程度较小。
排泄
单次口服300 mg放射性标记的图卡替尼后,粪便中回收了总放射性标记剂量的约86%(不变剂量的图卡替尼占给药剂量的16%),尿中回收了4.1%,在13天内总回收率达到90%给药后。在血浆中,约有76%的血浆放射性没有改变,有19%归因于鉴定出的代谢产物,约5%未分配。
特定人群
年龄(<65(n = 211);≥65(n = 27)),白蛋白(25至52 g / L),肌酸酐清除率(肌酸酐清除率[CLcr] 60至89 mL / min(n = 89); CLcr 30至59 mL / min(n = 5)),体重(41至138 kg)和种族(白人(n = 168),黑人(n = 53)或亚洲人(n = 10))没有对图卡替尼暴露量具有临床意义的影响。
肾功能不全
在轻度至中度肾功能不全患者(Cockcroft-Gault肌酐清除率:30至89 mL / min)中,未观察到图卡替尼药代动力学的临床显着差异。严重肾功能不全(肌酐清除率:<30 mL / min)对托卡替尼药代动力学的影响尚不清楚。
肝功能不全
轻度(Child-Pugh A)和中度(Child-Pugh B)肝损害对图卡替尼暴露无临床相关影响。 与具有正常肝功能的受试者相比,患有严重(Child-Pugh C)肝功能不全的受试者的图卡替尼AUC 0-INF增加了1.6倍。
药物相互作用研究
临床研究
表7:其他药物对TUKYSA的影响
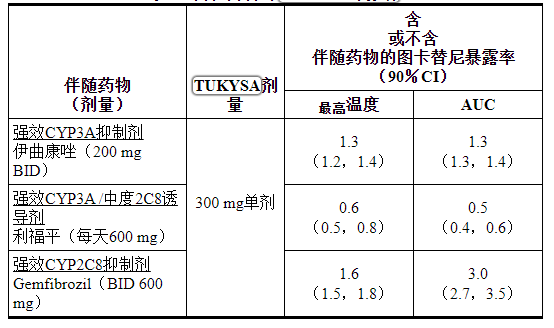
表8:TUKYSA对其他药物的影响
当与奥美拉唑(质子泵抑制剂)或甲苯磺丁酰胺(敏感的CYP2C9底物)并用时,未观察到图卡替尼药代动力学的临床显着差异。
体外研究
细胞色素P450(CYP)酶:图卡替尼是CYP2C8和CYP3A的可逆抑制剂和CYP3A的时间依赖性抑制剂,但不是CYP1A2,CYP2B6,CYP2C9,CYP2C19或CYP2D6的抑制剂。
尿苷二磷酸(UDP)-葡萄糖醛酸转移酶(UGT)酶:图卡替尼不是UGT1A1的抑制剂。
运输系统:图卡替尼是P-gp和BCRP的底物,但不是OAT1,OAT3,OCT1,OCT2,OATP1B1,OATP1B3,MATE1,MATE2-K或BSEP的底物。
图卡替尼抑制MATE1 / MATE2-K介导的二甲双胍转运和OCT2 / MATE1介导的肌酐转运。在临床研究中使用图卡替尼观察到的血清肌酐增加是由于通过OCT2和MATE1抑制了肌酐的肾小管分泌。
13毒理学
13.1致癌,诱变,生育力受损
尚未对图卡替尼进行致癌性研究。
在体外细菌反向突变(Ames)分析中,图卡替尼不具有致突变性。在体外染色体畸变试验或体内小鼠骨髓微核试验中,图卡替尼均无致死性。
尚未对动物进行生育力研究。在长达13周的重复剂量毒性研究中,在雌性大鼠中,剂量≥6 mg / kg /一天(基于AUC的推荐剂量,约为人体暴露量的0.1倍)。在雄性大鼠中,≥≥120 mg / kg /天(在基于AUC的推荐剂量下,人体暴露量的13倍)观察到睾丸的睾丸萎缩和水肿以及附睾中的少精子/生殖细胞碎片。
14临床研究
14.1 HER2阳性转移性乳腺癌
在612例HER2CLIMB(NCT02614794)患者中评估了TUKYSA联合曲妥珠单抗和卡培他滨的疗效(NCT02614794),这是一项随机(2:1),双盲,安慰剂对照试验。要求患者在新辅助药中单独或联合使用HER2阳性,不可切除的局部晚期或转移性乳腺癌,伴或不伴脑转移,并先用曲妥珠单抗,帕妥珠单抗和阿托曲妥珠单抗(T-DM1)单独或联合治疗,辅助或转移性环境。HER2阳性是基于登记之前或在中心实验室使用FDA批准的测试对新鲜档案组织进行测试后,HER2阳性被定义为HER2 IHC 3+或ISH阳性。
患有脑转移瘤的患者,包括具有进展性疾病或未经治疗的病变的患者,只要其神经学稳定且不需要立即放疗或手术,就符合资格。该试验排除了患有软脑膜疾病的患者。根据脑转移的存在或历史(是与否),东部合作肿瘤小组(ECOG)的表现状态(0对1)和地区(美国,加拿大或世界其他地区)对随机分组。
患者需要每天口服两次TUKYSA 300 mg或安慰剂,如果需要,在第1周期的第1天接受曲妥珠单抗负荷剂量8 mg / kg,然后在随后的每21天第1天的第1天维持维持剂量6 mg / kg,并给予卡培他滨在每个21天周期的第1天到第14天,每天两次口服1000 mg / m 2。在每个21天周期的第1天,皮下注射另一种曲妥珠单抗给药方案为600 mg。对患者进行治疗直至疾病进展或出现不可接受的毒性。在最初的24周中,每6周进行一次肿瘤评估,包括在基线存在或有脑转移史的患者进行脑MRI检查,之后每9周进行一次。
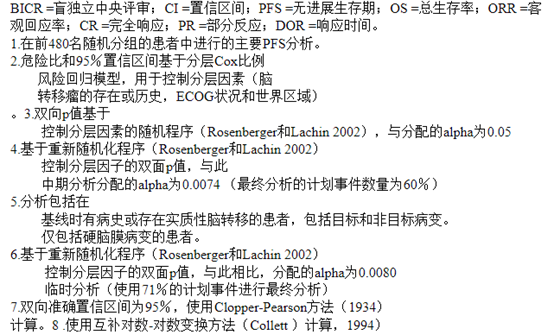
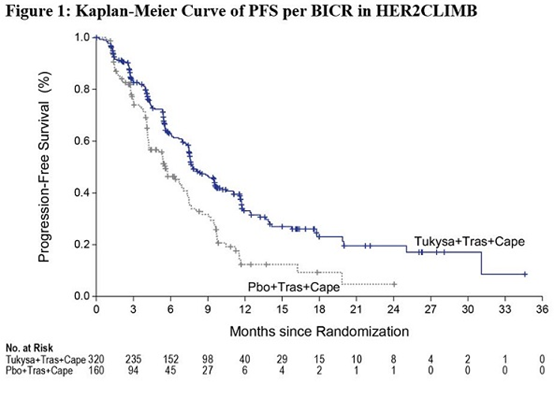
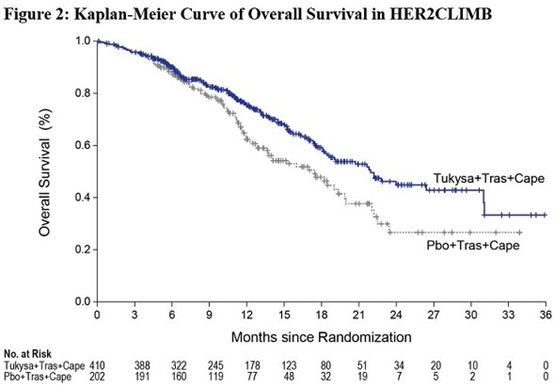
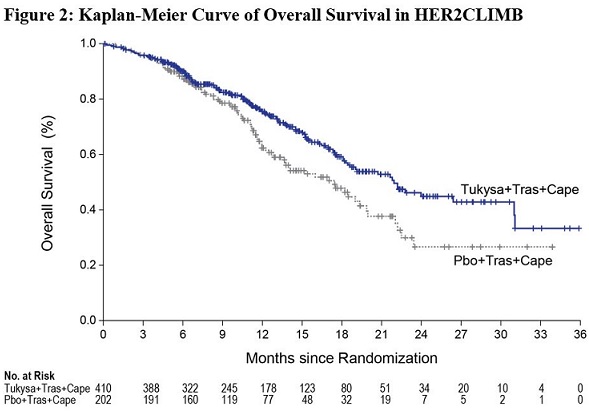
主要疗效结局指标是使用实体瘤反应评估标准(RECIST)v1.1通过盲独立独立评价(BICR)评估的前480名随机分组患者的无进展生存期(PFS)。在所有随机分组的患者中评估了其他疗效结局指标,包括总生存期(OS),有脑转移病史或存在脑转移病的患者中的PFS(PFS BrainMets),以及确定的客观缓解率(ORR)。
中位年龄是54岁(范围:22-82);116名(19%)患者年龄在65岁或以上。多数为白人(73%),女性(99%)和51%,其ECOG表现为1。60%患有雌激素和/或孕激素受体阳性疾病。48%的人有脑转移瘤的病史或病史;这些患者中,有23%未经治疗的脑转移瘤,40%经过治疗但稳定的脑转移瘤和37%有经过放射治疗但放射学进展的脑转移瘤。74%的患者发生内脏转移。在转移性环境中,患者接受过中位数的4线(范围2到17)以前的全身疗法,接受过中位的3线(范围1到14)以前的全身疗法。所有患者均接受过曲妥珠单抗和T-DM1治疗,除两名患者外均接受过帕妥珠单抗治疗。
疗效结果总结在表9和图1 和2中。在由分层因素(脑转移的存在或历史,ECOG状态,世界区域)和激素受体状态定义的患者亚组中,疗效结果是一致的。
表9:HER2CLIMB中的功效结果

16供应/存储和处理方式
16.1供应方式
TUKYSA 50 mg片剂以黄色,薄膜包衣的圆形片剂形式提供,其中包含50 mg的图卡替尼。每个平板电脑的凹处都有“ TUC”字样,另一侧则有“ 50”字样,包装如下:
50毫克片剂:75毫升瓶装60计数:NDC 51144-001-60
TUKYSA 150毫克片剂以包含150毫克曲妥替尼的黄色薄膜包衣椭圆形片剂形式提供。每个平板电脑的凹处都有“ TUC”字样,另一侧则有“ 150”字样,包装如下:
150毫克片剂:75毫升瓶装60计数:NDC 51144-002-60
150毫克片剂:150毫升瓶装120计数:NDC 51144-002-12
存放在20ºC至25ºC(68ºF至77ºF)的受控室温下;允许的温度偏移范围是15ºC至30ºC(59ºF至86ºF)[请参见USP控制的室温]。
仅在原始容器中分配患者。存放在原始容器中以防潮。每次打开后都要牢固地盖上盖子。请勿丢弃干燥剂。
打开后,请在3个月内使用。打开瓶子3个月后,丢弃所有未使用的药片。
17患者咨询信息
建议患者阅读FDA批准的患者标签(患者信息)。
腹泻
- 告知患者TUKYSA与严重腹泻有关。指导患者如何处理腹泻,如果肠管形态有任何变化,应立即告知其医护人员[请参阅警告和注意事项(5.1) ]。
肝毒性
- 告知患者TUKYSA与严重的肝毒性有关,应立即向医护人员报告肝功能不全的体征和症状[见警告和注意事项(5.2) ]。
胚胎-胎儿毒性
- 告知孕妇和有生殖风险的胎儿。劝告女性告知其已知或怀疑怀孕的健康护理人员[请参阅警告和注意事项(5.3)和特定人群的使用(8.1) ] 。
- 劝告有生殖潜力的女性在接受TUKYSA治疗期间以及最后一次给药后至少1周内使用有效的避孕方法(请参见“ 在特定人群中使用(8.3) ”)。
- 建议具有生殖潜力的女性伴侣的男性患者在接受TUKYSA治疗期间以及最后一次给药后至少1周内使用有效的避孕方法(请参见“ 在特定人群中使用(8.3) ”)。
- 有关妊娠和避孕的信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
哺乳期
- 劝告妇女在用TUKYSA治疗期间以及末次给药后至少1周内不要母乳喂养[参见在特定人群中使用(8.2) ]。有关泌乳信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。
不孕症
- 向具有生殖潜力的男性和女性建议TUKYSA可能会损害生育能力[请参见在特定人群中使用(8.3) ]。有关不育信息,请参阅曲妥珠单抗和卡培他滨的完整处方信息。

制造商:
Seattle Genetics,Inc. 博塞尔,华盛顿州98021
1-855-4SEAGENTUKYSA是

Seattle Genetics,Inc. 的商标,并且是Seattle Genetics,Inc.在美国的注册商标。
©2020 Seattle Genetics,Inc.,博塞尔,华盛顿州98021。保留所有权利。
主要显示面板
NDC 51144- 001 -60
Rx Only TM TUKYSA TM(图卡替尼)片剂50 mg *注意:将Tukysa分配并存放在原始容器中以防潮。西雅图遗传学® 60片*每片含50毫克tucatinib。建议剂量:请参阅处方信息。存放在受控的室温下,20°C至25°C(68°至77°F);允许的温度偏移范围是15°C至30°C(59°F至86°F) [请参阅USP控制的室温]。避免接触儿童打开后三个月,丢弃未使用的药片。西雅图遗传学公司制造
华盛顿州
博瑟尔 98021美国TUKYSA及其徽标是Seattle Genetics,Inc.的商标 。
©2020 Seattle Genetics,Inc.保留所有权利。美国印刷
1208-00
NDC 51144- 002 -60
Rx仅TUKYSA TM(图卡替尼)片剂150 mg *注意:将Tukysa分配并存储在原始容器中以防潮。西雅图遗传学® 60片*每片含150毫克tucatinib。建议剂量:请参阅处方信息。存放在受控的室温下,20°C至25°C(68°至77°F);允许的温度 偏移范围是15°C至30°C(59°F至86°F) [请参阅USP控制的室温]。避免接触儿童打开后三个月,丢弃未使用的药片。西雅图遗传学公司制造
华盛顿州
博瑟尔 98021美国TUKYSA及其徽标是Seattle Genetics,Inc.的商标 。
©2020 Seattle Genetics,Inc.保留所有权利。美国印刷
1200-00
【备注】以上内容仅供参考,不作为用药依据,详情请参照药品附带说明书。
-
本说明书来源于:美国FDA网站
温馨提醒:
①建议您用 谷歌浏览器 在电脑上或手机 打开以上链接,就可以自动翻译成简体中文,而且翻译的还比较准确。
②本说明书仅供参考,最新的说明书详见药品附带的说明书。
1 INDICATIONS AND USAGE
TUKYSA is indicated in combination with trastuzumab and capecitabine for treatment of adult patients with advanced unresectable or metastatic HER2-positive breast cancer, including patients with brain metastases, who have received one or more prior anti-HER2-based regimens in the metastatic setting.
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
The recommended dosage of TUKYSA is 300 mg taken orally twice daily in combination with trastuzumab and capecitabine until disease progression or unacceptable toxicity [see Clinical Studies (14)].
Advise patients to swallow TUKYSA tablets whole and not to chew, crush, or split prior to swallowing. Advise patients not to ingest tablet if it is broken, cracked, or not otherwise intact.
Advise patients to take TUKYSA approximately 12 hours apart and at the same time each day with or without a meal.
If the patient vomits or misses a dose of TUKYSA, instruct the patient to take the next dose at its usual scheduled time.
When given in combination with TUKYSA, the recommended dosage of capecitabine is 1000 mg/m2 orally twice daily taken within 30 minutes after a meal. TUKYSA and capecitabine can be taken at the same time. Refer to the Full Prescribing Information for trastuzumab and capecitabine for additional information.
2.2 Dosage Modifications for Adverse Reactions
The recommended TUKYSA dose reductions and dosage modifications for adverse reactions are provided in Tables 1 and 2. Refer to the Full Prescribing Information for trastuzumab and capecitabine for information about dosage modifications for these drugs.
Table 1: Recommended TUKYSA Dose Reductions for Adverse Reactions
Permanently discontinue TUKYSA in patients unable to tolerate 150 mg orally twice daily.
Table 2: Recommended TUKYSA Dosage Modifications for Adverse Reactions
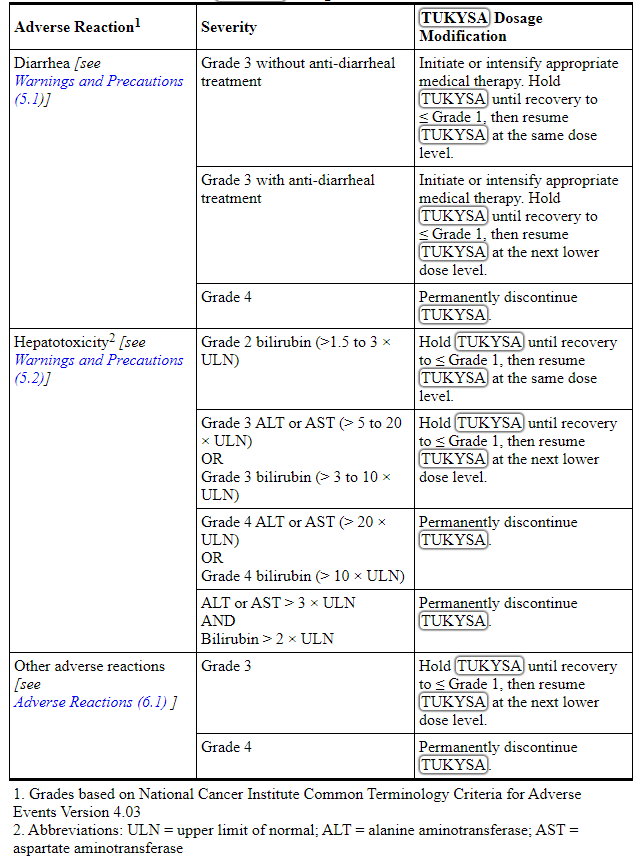
2.3 Dosage Modifications for Severe Hepatic Impairment
For patients with severe hepatic impairment (Child-Pugh C), reduce the recommended dosage to 200 mg orally twice daily [see Use in Specific Populations (8.7), Clinical Pharmacology (12.3)].
2.4 Dosage Modifications for Concomitant Use with Strong CYP2C8 Inhibitors
Avoid concomitant use of strong CYP2C8 inhibitors with TUKYSA. If concomitant use with a strong CYP2C8 inhibitor cannot be avoided, reduce the recommended dosage to 100 mg orally twice daily. After discontinuation of the strong CYP2C8 inhibitor for 3 elimination half-lives, resume the TUKYSA dose that was taken prior to initiating the inhibitor [see Drug Interactions (7.2), Clinical Pharmacology (12.3)].
3 DOSAGE FORMS AND STRENGTHS
Tablets:
- 50 mg: round, yellow, film-coated, debossed with “TUC” on one side and “50” on the other side.
- 150 mg: oval-shaped, yellow, film-coated, debossed with “TUC” on one side and “150” on the other side.
4 CONTRAINDICATIONS
None.
5 WARNINGS AND PRECAUTIONS
5.1 Diarrhea
TUKYSA can cause severe diarrhea including dehydration, hypotension, acute kidney injury, and death [see Adverse Reactions (6.1)]. In HER2CLIMB, 81% of patients who received TUKYSA experienced diarrhea, including 12% with Grade 3 diarrhea and 0.5% with Grade 4 diarrhea. Both patients who developed Grade 4 diarrhea subsequently died, with diarrhea as a contributor to death. The median time to onset of the first episode of diarrhea was 12 days and the median time to resolution was 8 days. Diarrhea led to dose reductions of TUKYSA in 6% of patients and discontinuation of TUKYSA in 1% of patients. Prophylactic use of antidiarrheal treatment was not required on HER2CLIMB.
If diarrhea occurs, administer antidiarrheal treatment as clinically indicated. Perform diagnostic tests as clinically indicated to exclude other causes of diarrhea. Based on the severity of the diarrhea, interrupt dose, then dose reduce or permanently discontinue TUKYSA [see Dosage and Administration (2.2)].
5.2 Hepatotoxicity
TUKYSA can cause severe hepatotoxicity [see Adverse Reactions (6.1)]. In HER2CLIMB, 8% of patients who received TUKYSA had an ALT increase > 5 × ULN, 6% had an AST increase > 5 × ULN, and 1.5% had a bilirubin increase > 3 × ULN (Grade ≥3). Hepatotoxicity led to dose reduction of TUKYSA in 8% of patients and discontinuation of TUKYSA in 1.5% of patients.
Monitor ALT, AST, and bilirubin prior to starting TUKYSA, every 3 weeks during treatment, and as clinically indicated. Based on the severity of hepatoxicity, interrupt dose, then dose reduce or permanently discontinue TUKYSA [see Dosage and Administration (2.2)].
5.3 Embryo-Fetal Toxicity
Based on findings from animal studies and its mechanism of action, TUKYSA can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, administration of tucatinib to pregnant rats and rabbits during organogenesis caused embryo-fetal mortality, reduced fetal weight and fetal abnormalities at maternal exposures ≥ 1.3 times the human exposure (AUC) at the recommended dose.
Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with TUKYSA and for at least 1 week after the last dose. Advise male patients with female partners of reproductive potential to use effective contraception during treatment with TUKYSA and for at least 1 week after the last dose [see Use in Specific Populations (8.1, 8.3)].
TUKYSA is used in combination with trastuzumab and capecitabine. Refer to the Full Prescribing Information of trastuzumab and capecitabine for pregnancy and contraception information.
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Diarrhea [see Warnings and Precautions (5.1)]
- Hepatotoxicity [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
HER2-Positive Metastatic Breast Cancer
HER2CLIMB
The safety of TUKYSA in combination with trastuzumab and capecitabine was evaluated in HER2CLIMB [see Clinical Studies (14)]. Patients received either TUKYSA 300 mg twice daily plus trastuzumab and capecitabine (n=404) or placebo plus trastuzumab and capecitabine (n=197). The median duration of treatment was 5.8 months (range: 3 days, 2.9 years) for the TUKYSA arm.
Serious adverse reactions occurred in 26% of patients who received TUKYSA. Serious adverse reactions in ≥ 2% of patients who received TUKYSA were diarrhea (4%), vomiting (2.5%), nausea (2%), abdominal pain (2%), and seizure (2%). Fatal adverse reactions occurred in 2% of patients who received TUKYSA including sudden death, sepsis, dehydration, and cardiogenic shock.
Adverse reactions leading to treatment discontinuation occurred in 6% of patients who received TUKYSA. Adverse reactions leading to treatment discontinuation of TUKYSA in ≥1% of patients were hepatotoxicity (1.5%) and diarrhea (1%).
Adverse reactions leading to dose reduction occurred in 21% of patients who received TUKYSA. Adverse reactions leading to dose reduction of TUKYSA in ≥2% of patients were hepatotoxicity (8%) and diarrhea (6%).
The most common adverse reactions in patients who received TUKYSA (≥20%) were diarrhea, palmar-plantar erythrodysesthesia, nausea, fatigue, hepatotoxicity, vomiting, stomatitis, decreased appetite, abdominal pain, headache, anemia, and rash.
Table 3 summarizes the adverse reactions in HER2CLIMB.
Table 3: Adverse Reactions (≥10%) in Patients Who Received TUKYSA and with a Difference Between Arms of ≥ 5% Compared to Placebo in HER2CLIMB (All Grades)
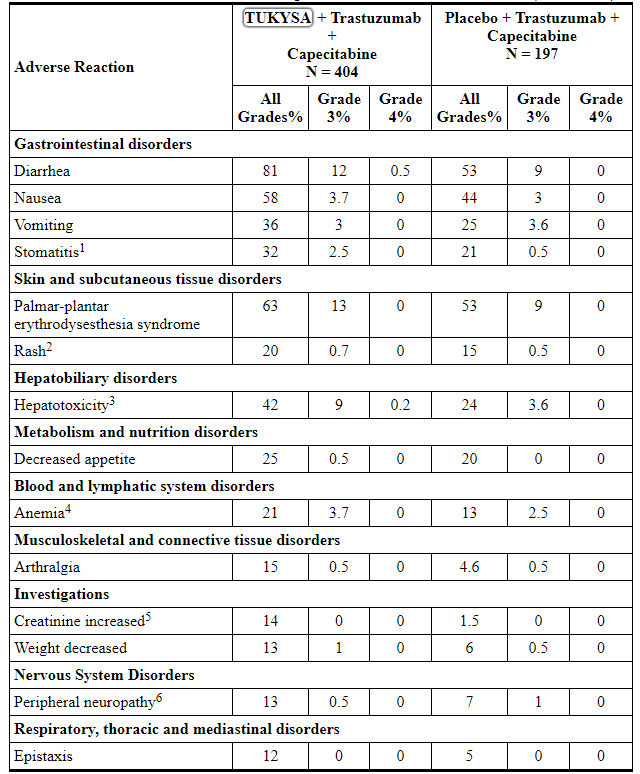
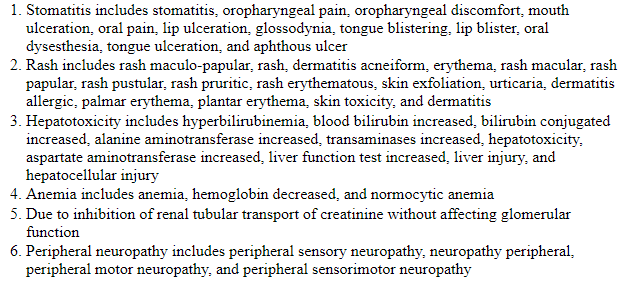
Table 4: Laboratory Abnormalities (≥20%) Worsening from Baseline in Patients Who Received TUKYSA and with a Difference of ≥5% Compared to Placebo in HER2CLIMB
Increased Creatinine
The mean increase in serum creatinine was 32% within the first 21 days of treatment with TUKYSA. The serum creatinine increases persisted throughout treatment and were reversible upon treatment completion. Consider alternative markers of renal function if persistent elevations in serum creatinine are observed [see Clinical Pharmacology (12.3)].
7 DRUG INTERACTIONS
7.1 Effects of Other Drugs on TUKYSA
Table 5 summarizes the effect of other drugs on TUKYSA.
Table 5: Drug Interactions that Affect TUKYSA
7.2 Effects of TUKYSA on Other Drugs
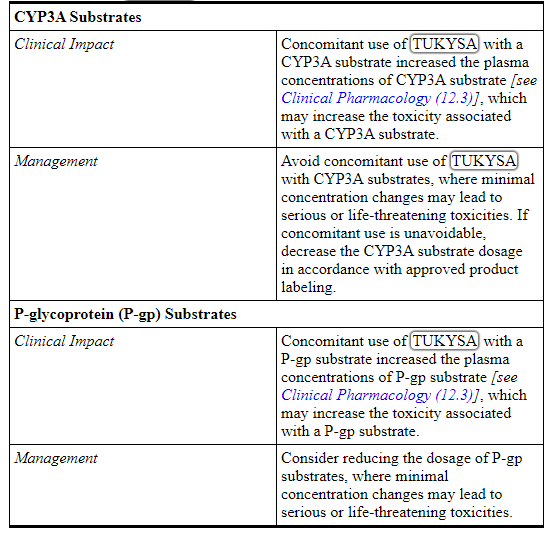
Table 6 summarizes the effect of TUKYSA on other drugs.
Table 6: TUKYSA Drug Interactions that Affect
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
TUKYSA is used in combination with trastuzumab and capecitabine. Refer to the Full Prescribing Information of trastuzumab and capecitabine for pregnancy information.
Based on findings in animals and its mechanism of action, TUKYSA can cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. There are no available human data on TUKYSA use in pregnant women to inform a drug-associated risk. In animal reproduction studies, administration of tucatinib to pregnant rats and rabbits during organogenesis resulted in embryo-fetal mortality, reduced fetal weight and fetal abnormalities at maternal exposures ≥ 1.3 times the human exposure (AUC) at the recommended dose (see Data). Advise pregnant women and females of reproductive potential of the potential risk to the fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2%-4% and 15%-20%, respectively.
Data
Animal Data
In pilot embryo-fetal development studies, pregnant rats and rabbits received oral doses of tucatinib up to 150 mg/kg/day during the period of organogenesis.
In rats, oral administration of tucatinib resulted in maternal toxicity (body weight loss, reduced body weight gain, low food consumption) at doses ≥ 90 mg/kg/day. Fetal effects included reduced number of live fetuses, decreased fetal weight, and fetal abnormalities (increase in skeletal variations, incomplete ossification) at ≥ 90 mg/kg/day (approximately 3.5 times the human exposure at the recommended dose based on AUC).
In rabbits, oral administration of tucatinib resulted in increased resorptions, decreased percentages of live fetuses, and skeletal, visceral, and external malformations in fetuses at doses ≥ 90 mg/kg/day (1.3 times the human exposure at the recommended dose based on AUC). Fetal abnormalities included domed head, brain dilation, incomplete ossification of frontal and parietal bones, and a hole in the parietal bone.
8.2 Lactation
Risk Summary
TUKYSA is used in combination with trastuzumab and capecitabine. Refer to the Full Prescribing Information of trastuzumab and capecitabine for lactation information.
There are no data on the presence of tucatinib or its metabolites in human or animal milk or its effects on the breastfed child or on milk production. Because of the potential for serious adverse reactions in a breastfed child, advise women not to breastfeed during treatment with TUKYSA and for at least 1 week after the last dose.
8.3 Females and Males of Reproductive Potential
TUKYSA can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)]. TUKYSA is used in combination with trastuzumab and capecitabine. Refer to the Full Prescribing Information of trastuzumab and capecitabine for contraception and infertility information.
Pregnancy Testing
Verify the pregnancy status of females of reproductive potential prior to initiating treatment with TUKYSA.
Contraception
Females
Advise females of reproductive potential to use effective contraception during treatment with TUKYSA and for at least 1 week after the last dose.
Males
Advise male patients with female partners of reproductive potential to use effective contraception during treatment with TUKYSA and for at least 1 week after the last dose.
Infertility
Based on findings from animal studies, TUKYSA may impair male and female fertility [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of TUKYSA in pediatric patients have not been established.
8.5 Geriatric Use
In HER2CLIMB, 82 patients who received TUKYSA were ≥ 65 years, of whom 8 patients were ≥ 75 years. The incidence of serious adverse reactions in those receiving TUKYSA was 34% in patients ≥ 65 years compared to 24% in patients <65 years. The most frequent serious adverse reactions in patients who received TUKYSA and ≥ 65 years were diarrhea (9%), vomiting (6%), and nausea (5%). There were no observed overall differences in the effectiveness of TUKYSA in patients ≥ 65 years compared to younger patients. There were too few patients ≥75 years to assess differences in effectiveness or safety.
8.6 Renal Impairment
The use of TUKYSA in combination with capecitabine and trastuzumab is not recommended in patients with severe renal impairment (CLcr < 30 mL/min estimated by Cockcroft-Gault Equation), because capecitabine is contraindicated in patients with severe renal impairment. Refer to the Full Prescribing Information of capecitabine for additional information in severe renal impairment.
No dose adjustment is recommended for patients with mild or moderate renal impairment (creatinine clearance [CLcr] 30 to 89 mL/min).
8.7 Hepatic Impairment
Tucatinib exposure is increased in patients with severe hepatic impairment (Child-Pugh C). Reduce the dose of TUKYSA for patients with severe (Child-Pugh C) hepatic impairment [see Dosage and Administration (2.3), Clinical Pharmacology (12.3)].
No dose adjustment for TUKYSA is required for patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment.
11 DESCRIPTION
Tucatinib is a kinase inhibitor. The chemical name is (N4-(4-([1,2,4]triazolo[1,5-a]pyridin-7-yloxy)-3-methylphenyl)-N6-(4,4-dimethyl-4,5-dihydrooxazol-2-yl)quinazoline-4,6-diamine. The molecular formula is C26H24N8O2 and the molecular weight is 480.52 g/mol. The chemical structure is as follows:
TUKYSA (tucatinib) is supplied as 50 mg and 150 mg film-coated tablets for oral use and contain the following inactive ingredients:
Tablet core: copovidone, crospovidone, sodium chloride, potassium chloride, sodium bicarbonate, colloidal silicon dioxide, magnesium stearate, and microcrystalline cellulose.
Coating: yellow film coat: polyvinyl alcohol, titanium dioxide, macrogol/polyethylene glycol, talc, and yellow iron oxide non-irradiated.
Each TUKYSA 50 mg tablet contains 10.10 mg (0.258 mEq) potassium and 9.21 mg (0.401 mEq) sodium.
Each TUKYSA 150 mg tablet contains 30.29 mg (0.775 mEq) potassium and 27.64 mg (1.202 mEq) sodium.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Tucatinib is a tyrosine kinase inhibitor of HER2. In vitro, tucatinib inhibits phosphorylation of HER2 and HER3, resulting in inhibition of downstream MAPK and AKT signaling and cell proliferation, and showed anti-tumor activity in HER2 expressing tumor cells. In vivo, tucatinib inhibited the growth of HER2 expressing tumors. The combination of tucatinib and trastuzumab showed increased anti-tumor activity in vitro and in vivo compared to either drug alone.
12.2 Pharmacodynamics
Exposure Response Relationship
Tucatinib exposure-response relationships and the time course of pharmacodynamics response have not been fully characterized.
Cardiac Electrophysiology
No large mean increase in QTc (i.e., > 20 ms) was detected following treatment with TUKYSA at the recommended dose of 300 mg taken orally twice daily.
12.3 Pharmacokinetics
Tucatinib AUC0-INF and Cmax increases proportionally over a dosage range from 50 mg to 300 mg (0.17 to 1 times the approved recommended dosage). Tucatinib exhibited 1.7-fold accumulation for AUC and 1.5-fold accumulation for Cmax following administration of TUKYSA 300 mg twice daily for 14 days. Time to steady state was approximately 4 days.
Absorption
The median time to peak plasma concentration of tucatinib was approximately 2 hours (range 1 to 4 hours).
Effects of Food
Following administration of a single oral dose of TUKYSA in 11 subjects after a high-fat meal (approximately 58% fat, 26% carbohydrate, and 16% protein), the mean AUC0-INF increased by 1.5-fold, the Tmax shifted from 1.5 hours to 4 hours, and Cmax was unaltered. The effect of food on the pharmacokinetics of tucatinib was not clinically meaningful.
Distribution
The geometric mean (CV%) apparent volume of distribution of tucatinib was approximately 1670 L (66%). The plasma protein binding was 97.1% at clinically relevant concentrations.
Elimination
The geometric mean (CV%) half-life of tucatinib was approximately 8.5 (21%) hours and apparent clearance was 148 L/h (55%).
Metabolism
Tucatinib is metabolized primarily by CYP2C8 and to a lesser extent via CYP3A.
Excretion
Following a single oral dose of 300 mg radiolabeled tucatinib, approximately 86% of the total radiolabeled dose was recovered in feces (16% of the administered dose as unchanged tucatinib) and 4.1% in urine with an overall total recovery of 90% within 13 days post-dose. In plasma, approximately 76% of the plasma radioactivity was unchanged, 19% was attributed to identified metabolites, and approximately 5% was unassigned.
Specific Populations
Age (< 65 (n =211); ≥ 65 (n = 27)), albumin (25 to 52 g/L), creatinine clearance (creatinine clearance [CLcr] 60 to 89 mL/min (n = 89); CLcr 30 to 59 mL/min (n = 5)), body weight (41 to 138 kg), and race (White (n=168), Black (n=53), or Asian (n=10)) did not have a clinically meaningful effect on tucatinib exposure.
Renal Impairment
No clinically significant differences in the pharmacokinetics of tucatinib were observed in patients with mild to moderate renal impairment (creatinine clearance: 30 to 89 mL/min by Cockcroft-Gault). The effect of severe renal impairment (creatinine clearance: < 30 mL/min) on the pharmacokinetics of tucatinib is unknown.
Hepatic Impairment
Mild (Child-Pugh A) and moderate (Child-Pugh B) hepatic impairment had no clinically relevant effect on tucatinib exposure. Tucatinib AUC0-INF was increased by 1.6 fold in subjects with severe (Child-Pugh C) hepatic impairment compared to subjects with normal hepatic function.
Drug Interaction Studies
Clinical Studies
Table 7: Effect of Other Drugs on TUKYSA
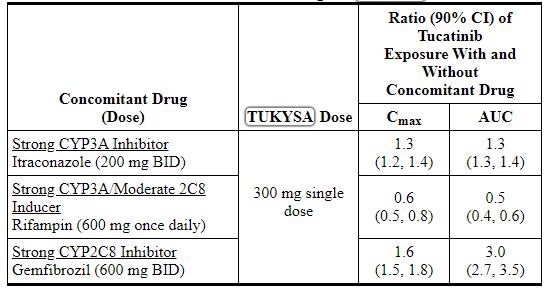
Table 8: Effect of TUKYSA on Other Drugs
No clinically significant difference in the pharmacokinetics of tucatinib were observed when used concomitantly with omeprazole (proton pump inhibitor) or tolbutamide (sensitive CYP2C9 substrate).
In Vitro Studies
Cytochrome P450 (CYP) Enzymes: Tucatinib is a reversible inhibitor of CYP2C8 and CYP3A and a time-dependent inhibitor of CYP3A, but is not an inhibitor of CYP1A2, CYP2B6, CYP2C9, CYP2C19, or CYP2D6.
Uridine diphosphate (UDP)-glucuronosyl transferase (UGT) Enzymes: Tucatinib is not an inhibitor of UGT1A1.
Transporter Systems: Tucatinib is a substrate of P-gp and BCRP, but is not a substrate of OAT1, OAT3, OCT1, OCT2, OATP1B1, OATP1B3, MATE1, MATE2-K, or BSEP.
Tucatinib inhibits MATE1/MATE2-K-mediated transport of metformin and OCT2/MATE1-mediated transport of creatinine. The observed serum creatinine increase in clinical studies with tucatinib is due to inhibition of tubular secretion of creatinine via OCT2 and MATE1.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with tucatinib.
Tucatinib was not mutagenic in an in vitro bacterial reverse mutation (Ames) assay. Tucatinib was not clastogenic in either an in vitro chromosome aberration assay or an in vivo mouse bone marrow micronucleus assay.
Fertility studies in animals have not been conducted. In repeat-dose toxicity studies up to 13 weeks duration, decreased corpora lutea/corpus luteum cyst, increased interstitial cells of the ovary, atrophy of the uterus, and mucification of the vagina were observed in female rats at doses ≥ 6 mg/kg/day (approximately 0.1 times the human exposure at the recommended dose based on AUC). Atrophy and edema of the testes and oligospermia/germ cell debris in the epididymides were observed in male rats at ≥ 120 mg/kg/day (approximately 13 times the human exposure at the recommended dose based on AUC).
14 CLINICAL STUDIES
14.1 HER2-Positive Metastatic Breast Cancer
The efficacy of TUKYSA in combination with trastuzumab and capecitabine was evaluated in 612 patients in HER2CLIMB (NCT02614794), a randomized (2:1), double-blind, placebo-controlled trial. Patients were required to have HER2-positive, unresectable locally advanced or metastatic breast cancer, with or without brain metastases, and prior treatment with trastuzumab, pertuzumab, and ado-trastuzumab emtansine (T-DM1) separately or in combination, in the neoadjuvant, adjuvant or metastatic setting. HER2 positivity was based on archival or fresh tissue tested with an FDA-approved test at a central laboratory prior to enrollment with HER2 positivity defined as HER2 IHC 3+ or ISH positive.
Patients with brain metastases, including those with progressing or untreated lesions, were eligible provided they were neurologically stable and did not require immediate radiation or surgery. The trial excluded patients with leptomeningeal disease. Randomization was stratified by the presence or history of brain metastases (yes vs. no), Eastern Cooperative Oncology Group (ECOG) performance status (0 vs. 1), and region (U.S., Canada, or rest of world).
Patients received TUKYSA 300 mg or placebo orally twice daily with a trastuzumab loading dose of 8 mg/kg on Day 1 of Cycle 1 if needed and then a maintenance dose of 6 mg/kg on Day 1 of every 21-day cycle thereafter and capecitabine 1000 mg/m2 orally twice daily on Days 1 through 14 of every 21-day cycle. An alternate trastuzumab dosing regimen was 600 mg administered subcutaneously on Day 1 of every 21-day cycle. Patients were treated until disease progression or unacceptable toxicity. Tumor assessments, including brain-MRI in patients with presence or history of brain metastases at baseline, occurred every 6 weeks for the first 24 weeks and every 9 weeks thereafter.
The major efficacy outcome measure was progression-free survival (PFS) in the first 480 randomized patients assessed by blinded independent central review (BICR) using Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. Additional efficacy outcome measures were evaluated in all randomized patients and included overall survival (OS), PFS among patients with a history or presence of brain metastases (PFSBrainMets), and confirmed objective response rate (ORR).
The median age was 54 years (range: 22 - 82); 116 (19%) patients were age 65 or older. The majority were White (73%) and female (99%) and 51% had an ECOG performance status of 1. Sixty percent had estrogen and/or progesterone receptor-positive disease. Forty-eight percent had a presence or history of brain metastases; of these patients, 23% had untreated brain metastases, 40% had treated but stable brain metastases, and 37% had treated but radiographically progressing brain metastases. Seventy-four percent of patients had visceral metastases. Patients had received a median of 4 (range, 2 to 17) prior lines of systemic therapy and a median of 3 (range, 1 to 14) prior lines of systemic therapy in the metastatic setting. All patients received prior trastuzumab and T-DM1 and all but two patients had prior pertuzumab.
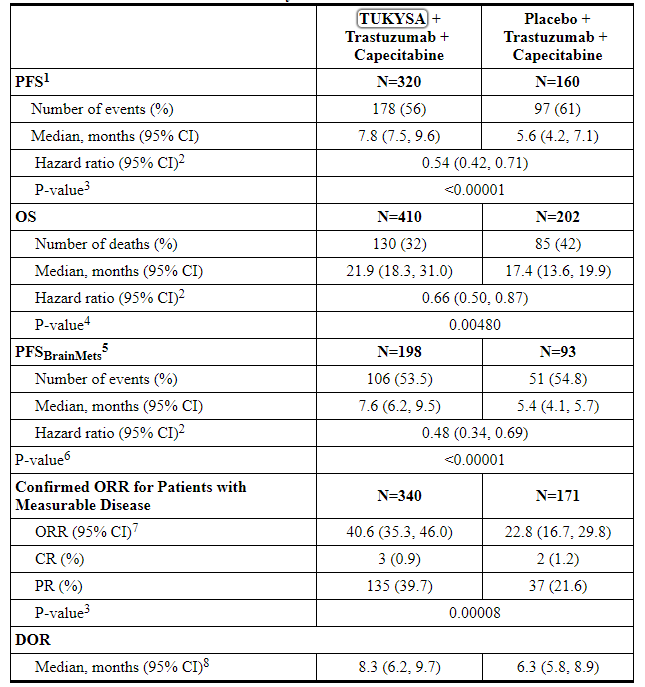
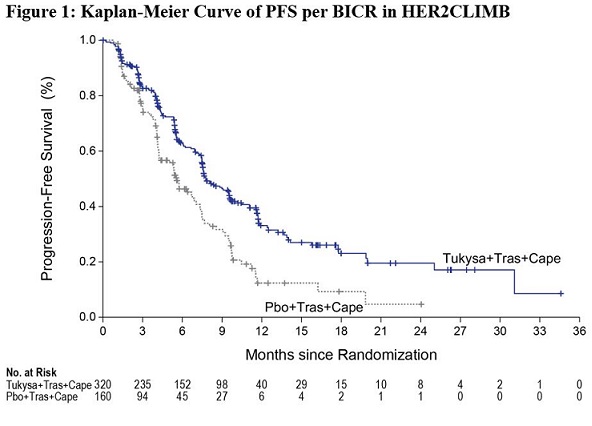
Efficacy results are summarized in Table 9 and Figure 1 and 2. Efficacy results were consistent across patient subgroups defined by stratification factors (presence or history of brain metastases, ECOG status, region of world) and hormone receptor status.
Table 9: Efficacy Results in HER2CLIMB
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
TUKYSA 50 mg tablets are supplied as yellow, film-coated, round tablets containing 50 mg of tucatinib. Each tablet is debossed with “TUC” on one side and “50” on the other side, and is packaged as follows:
50 mg tablets: 60 count in 75 cc bottle: NDC 51144-001-60
TUKYSA 150 mg tablets are supplied as yellow, film-coated, oval-shaped tablets containing 150 mg of tucatinib. Each tablet is debossed with “TUC” on one side and “150” on the other side, and is packaged as follows:
150 mg tablets: 60 count in 75 cc bottle: NDC 51144-002-60
150 mg tablets: 120 count in 150 cc bottle: NDC 51144-002-12
Store at controlled room temperature, 20ºC to 25ºC (68ºF to 77ºF); excursions permitted from 15ºC to 30ºC (59ºF to 86ºF) [see USP Controlled Room Temperature].
Dispense to patient in original container only. Store in original container to protect from moisture. Replace cap securely each time after opening. Do not discard desiccant.
Once opened, use within 3 months. Discard any unused tablets 3 months after opening the bottle.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Diarrhea
- Inform patients that TUKYSA has been associated with severe diarrhea. Instruct patients on how to manage diarrhea and to inform their healthcare provider immediately if there is any change in bowel patterns [see Warnings and Precautions (5.1)].
Hepatotoxicity
- Inform patients that TUKYSA has been associated with severe hepatotoxicity and that they should report signs and symptoms of liver dysfunction to their healthcare provider immediately [see Warnings and Precautions (5.2)].
Embryo-Fetal Toxicity
- Inform pregnant women and females of reproductive potential of the risk to a fetus. Advise females to inform their healthcare provider of a known or suspected pregnancy [see Warnings and Precautions (5.3) and Use in Specific Populations (8.1)].
- Advise females of reproductive potential to use effective contraception during treatment with TUKYSA and for at least 1 week after the last dose [see Use in Specific Populations (8.3)].
- Advise male patients with female partners of reproductive potential to use effective contraception during treatment with TUKYSA and for at least 1 week after the last dose [see Use in Specific Populations (8.3)].
- Refer to the Full Prescribing Information of trastuzumab and capecitabine for pregnancy and contraception information.
Lactation
- Advise women not to breastfeed during treatment with TUKYSA and for at least 1 week after the last dose [see Use in Specific Populations (8.2)]. Refer to the Full Prescribing Information of trastuzumab and capecitabine for lactation information.
Infertility
- Advise males and females of reproductive potential that TUKYSA may impair fertility [see Use in Specific Populations (8.3)]. Refer to the Full Prescribing Information of trastuzumab and capecitabine for infertility information.

Manufactured by:
Seattle Genetics, Inc.
Bothell, WA 98021
1-855-4SEAGENTUKYSA is a trademark, and Seattle Genetics and

are US registered trademarks of Seattle Genetics, Inc.
© 2020 Seattle Genetics, Inc., Bothell, WA 98021. All rights reserved.
PRINCIPAL DISPLAY PANEL
NDC 51144-001-60
Rx OnlyTM
TUKYSATM
(tucatinib) tablets
50 mg*
Attention: Dispense and store Tukysa
in original container to protect from moisture.
SeattleGenetics®
60 Tablets
* Each tablet contains 50 mg tucatinib.
Recommended Dosage: See prescribing information
Store at controlled room temperature,
20°C to 25°C (68° to 77°F); excursions
permitted from 15°C to 30°C (59°F to 86°F)
[see USP Controlled Room Temperature].
KEEP OUT OF REACH OF CHILDREN
Discard unused tablets 3 months after opening.
Mfg by Seattle Genetics, Inc.
Bothell, WA 98021 USATUKYSA and its logo are trademarks of Seattle Genetics, Inc.
©2020 Seattle Genetics, Inc.All rights reserved. Printed in USA
1208-00
NDC 51144-002-60
Rx Only
TUKYSATM
(tucatinib) tablets
150 mg*
Attention: Dispense and store Tukysa
in original container to protect from moisture.
SeattleGenetics®
60 Tablets
* Each tablet contains 150 mg tucatinib.
Recommended Dosage: See prescribing information
Store at controlled room temperature,
20°C to 25°C (68° to 77°F); excursions
permitted from 15°C to 30°C (59°F to 86°F)
[see USP Controlled Room Temperature].
KEEP OUT OF REACH OF CHILDREN
Discard unused tablets 3 months after opening.
Mfg by Seattle Genetics, Inc.
Bothell, WA 98021 USATUKYSA and its logo are trademarks of Seattle Genetics, Inc.
©2020 Seattle Genetics, Inc.All rights reserved. Printed in USA
1200-00
【备注】以上内容仅供参考,不作为用药依据,详情请参照药品附带说明书。