商品详情
返回产品目录


商品包装及说明书因厂家更换频繁,如有不符以实物为主
伊匹木单抗注射液
国际零售参考价:¥**/瓶
-
温馨提醒:本说明书仅供参考,最新的说明书详见药品附带的说明书。
警告:免疫介导的不良反应
YERVOY可能导致严重和致命的免疫介导的不良反应。这些免疫介导的反应可能涉及任何器官系统。然而,最常见的严重的免疫介导的不良反应是小肠结肠炎,肝炎,皮炎(包括中毒性表皮坏死溶解),神经病和内分泌病。这些免疫介导的反应大多数最初在治疗过程中表现出来。然而,少数人在停药后数周至数月出现。
永久终止YERVOY并开始全身性大剂量糖皮质激素治疗以应对严重的免疫介导反应[参见剂量和用法(2.5) ]。
在基线和每次给药前评估患者的小肠结肠炎,皮炎,神经病和内分泌病的体征和症状,并评估临床化学,包括肝功能检查,促肾上腺皮质激素(ACTH)水平和甲状腺功能检查[参见警告和注意事项(5.1),5.2,5.3,5.4,5.5) ]。
1适应症和用途
1.1不可切除或转移性黑色素瘤
YERVOY适用于成人和儿童患者(12岁及以上)不可切除或转移性黑色素瘤的治疗[见临床研究(14.1) ]。
1.2黑色素瘤的辅助治疗
YERVOY可以辅助治疗皮肤黑色素瘤患者,其病灶涉及超过1 mm的局部淋巴结,并且已进行了完全切除,包括全淋巴结清扫术[见临床研究(14.2) ]。
1.3晚期肾细胞癌
YERVOY与nivolumab联合使用,可用于治疗中度或低风险,先前未治疗的晚期肾细胞癌(RCC)[参见临床研究(14.3) ]。
1.4高微卫星不稳定性(MSI-H)或错配修复缺陷(dMMR)转移性大肠癌
YERVOY与nivolumab联合使用,可用于治疗12岁及以上的微卫星不稳定性高(MSI-H)或错配修复缺陷(dMMR)转移性结直肠癌(CRC)的成年和小儿患者氟嘧啶,奥沙利铂和伊立替康治疗[见临床研究(14.4) ]。该指示根据总体响应率和响应时间在加速批准下获得批准。对于该适应症的持续批准可能取决于验证试验中对临床益处的验证和描述。
2用法用量
2.1不可切除或转移性黑色素瘤的推荐剂量
YERVOY的推荐剂量为每3周90分钟静脉内(IV)施用3 mg / kg,最多4剂。如果发生毒性反应,可以延迟剂量,但是所有治疗都必须在首次给药后的16周内进行[见临床研究(14.1) ]。
2.2辅助治疗黑色素瘤的推荐剂量
推荐的YERVOY剂量为每3周90分钟静脉输注10 mg / kg,共4剂,然后每12周10 mg / kg,持续3年[见临床研究(14.2) ]。如果发生毒性,则省略剂量,不要延迟。
2.3 RCC的推荐剂量
YERVOY与nivolumab的推荐剂量是在30分钟内以静脉输注的方式将nivolumab 3 mg / kg给药,然后在同一天的30分钟内以静脉输注的方式将YERVOY 1 mg / kg进行给药,每3周一次,共4剂[参见临床研究(14.3) ]。完成4剂联合用药后,将nivolumab作为单一药物给药,可以:
• 每2周240毫克,或
• 每4周480毫克
在30分钟内静脉输注,直至疾病进展或出现不可接受的毒性。在开始使用之前,请复查nivolumab的处方信息。
2.4大肠癌的推荐剂量
建议的YERVOY剂量为:
• YERVOY在同一天尼伏鲁单抗给药后的30分钟内,静脉输注1 mg / kg,每3周一次,最多3剂,直至4剂,直到出现无法忍受的毒性或疾病进展[参见临床研究(14.4) ]。在开始使用之前,请复查nivolumab的处方信息。
2.5建议的剂量修改
表1中提供了有关YERVOY修饰的建议。当将YERVOY与nivolumab联合使用时,如果不使用YERVOY,也应不使用nivolumab。查看尼伏鲁单抗的处方信息,以获取建议的剂量调整。
有轻度或中度输液反应的患者中断或减慢输液速度。有严重或危及生命的输注反应的患者停药。
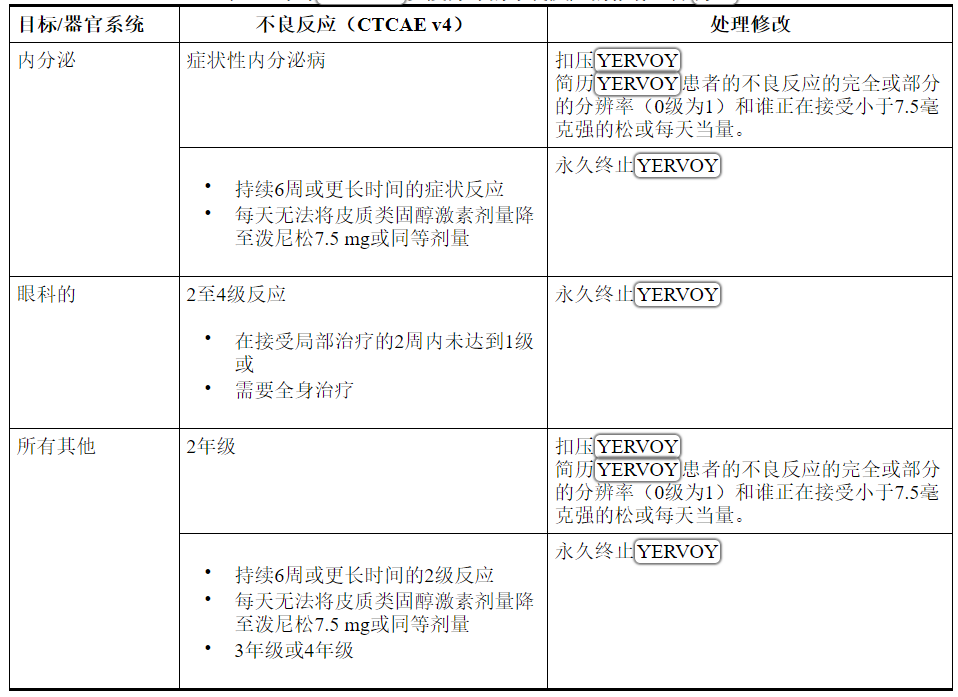
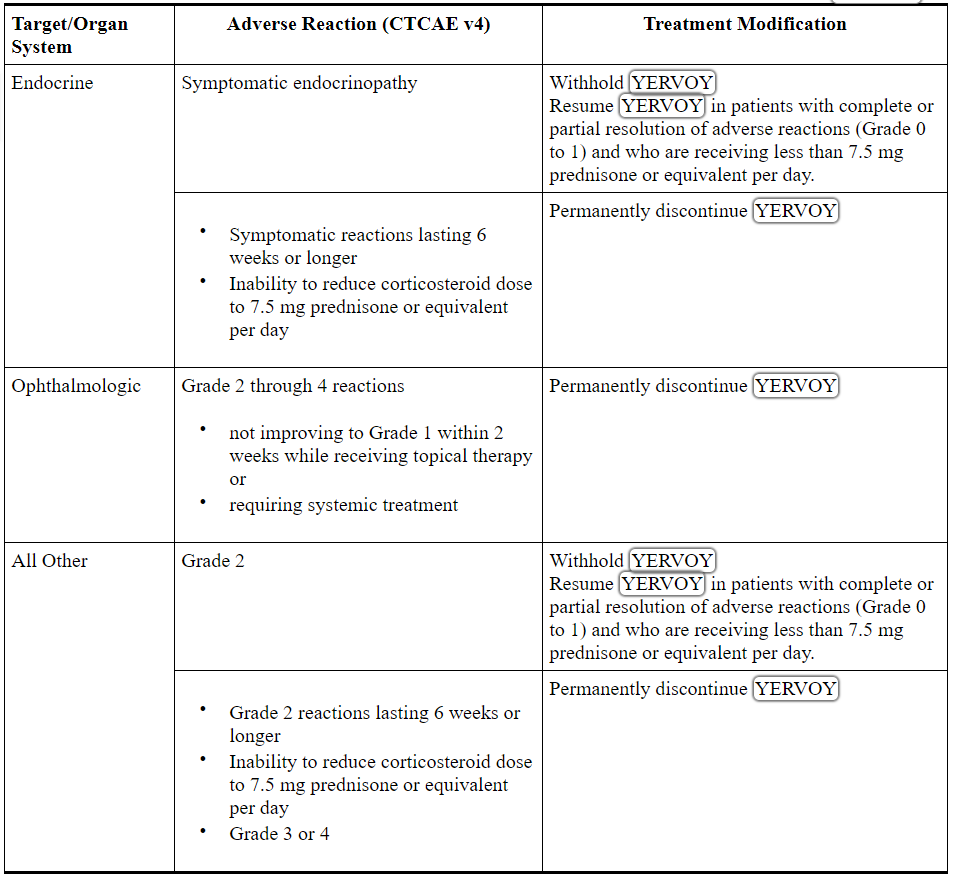
表1:针对YERVOY免疫介导的不良反应的推荐治疗方法
2.6准备和管理
• 请勿摇动产品。
• 给药前目视检查肠胃外药品是否有颗粒物质和变色。如果溶液浑浊,明显变色(溶液可能呈浅黄色)或有半透明至白色的无定形颗粒外,则应丢弃小瓶。
溶液制备
• 准备输液前,让小瓶在室温下静置约5分钟。
• 取出所需量的耶尔沃伊并转移到静脉注射袋中。
• 用0.9%氯化钠注射液(USP)或5%葡萄糖注射液(USP)稀释,以制备最终浓度为1 mg / mL至2 mg / mL的稀释溶液。轻轻颠倒混合稀释的溶液。
• 将稀释后的溶液在冷藏(2°C至8°C,36°F至46°F)或室温(20°C至25°C,68°F至77°F)下保存不超过24小时。
• 丢弃部分用过的小瓶或空瓶的YERVOY。
管理说明
• 请勿将YERVOY与其他药品混合或作为输注剂使用。
• 每次给药后,用0.9%氯化钠注射液USP或5%葡萄糖注射液USP冲洗静脉管线。
• 通过包含无菌,无热原,低蛋白结合的在线过滤器的静脉输液管,在90分钟内施用稀释液。
当与nivolumab联合给药时,先注入nivolumab,然后在同一天注射YERVOY。每次使用输液袋和过滤器。
3剂型和强度
注射剂:一次使用的小瓶中,澄清至微乳白色,无色至浅黄色溶液为50 mg / 10 mL(5 mg / mL)和200 mg / 40 mL(5 mg / mL)。
4禁忌症
没有。
5警告和注意事项
YERVOY可能导致严重且致命的免疫介导反应[请参阅盒装警告 ]。
5.1免疫介导的小肠结肠炎/结肠炎
YERVOY可能会发生免疫介导的小肠结肠炎,包括致命病例。
监测患者是否有小肠结肠炎(例如腹泻,腹痛,粘液或便血,发烧或不发烧)和肠穿孔(例如腹膜体征和肠梗阻)的体征和症状。在有症状的患者中,应排除感染性病因,并考虑对持续或严重症状进行内镜检查。皮质类固醇难治性免疫介导的结肠炎患者中已有巨细胞病毒(CMV)感染/再激活的报道。在皮质类固醇难治性结肠炎的情况下,请考虑重复进行感染性检查以排除其他病因。如果排除其他原因,应在皮质类固醇难治性免疫介导的结肠炎中考虑在皮质类固醇治疗中添加替代性免疫抑制剂,或替代皮质类固醇治疗。
重度小肠结肠炎患者应永久停用YERVOY,并以1至2 mg / kg /天的泼尼松或同等剂量开始全身性皮质类固醇激素治疗。改善至1级或以下后,开始逐渐降低皮质类固醇激素水平,并持续降低锥度至少1个月。在临床试验中,某些患者皮质类固醇激素逐渐减少导致小肠结肠炎的复发或症状加重。考虑排除抗TNF或其他免疫抑制剂,以治疗对全身性皮质类固醇无反应的免疫介导的小肠结肠炎,如果排除其他原因,则可在3至5天内或症状改善后复发。
中度小肠结肠炎不使用YERVOY剂量;进行抗腹泻治疗,如果持续治疗超过1周,则以0.5毫克/千克/天的泼尼松或同等剂量开始使用全身性皮质类固醇[见剂量和给药方法(2.5) ]。
YERVOY作为单一代理
转移性黑色素瘤
在MDX010-20(NCT00094653)中接受YERVOY 3 mg / kg的患者,严重的,危及生命的或致命的(腹泻超过基线的7个或更多大便,发烧,肠梗阻,腹膜征; 3至5级)是免疫介导的小肠结肠炎34例接受YERVOY治疗的患者(7%)发生中度肠炎(中度腹泻,基线以上最多有6凳大便,腹痛,粘液或便血; 2级),小肠结肠炎发生于28例接受YERVOY治疗的患者(5%)。在所有接受YERVOY治疗的患者(n = 511)中,有5例(1%)出现了肠穿孔,有4例(0.8%)因并发症而死亡,还有26例(5%)因重症小肠结肠炎住院。
3至5级小肠结肠炎的发作中位时间为1.7个月(范围:11天至3.1个月),而2级小肠结肠炎的中位发作时间为1.4个月(范围:2天至4.3个月)。
29例(35%至5级小肠结肠炎患者)接受了大剂量(每天泼尼松≥40毫克当量)皮质类固醇的治疗,中位数剂量为泼尼松每天80毫克或同等剂量;中位治疗时间为16天(最长3.2个月),然后进行皮质类固醇锥度治疗。在28例中度小肠结肠炎患者中,46%的患者未接受全身性皮质类固醇激素治疗,29%的患者接受了每天<40 mg泼尼松或同等剂量的药物治疗,中位时间为1.2个月,25%的患者接受大剂量皮质类固醇激素治疗,糖皮质激素减量前10天的中位数持续时间。在对皮质类固醇反应不足后,对62例中度,重度或危及生命的免疫介导小肠结肠炎患者中的5名(8%)给予了英夫利昔单抗。
在34位3至5级小肠结肠炎患者中,有74%的患者可以完全缓解,3%的患者达到2级严重程度,而24%的患者没有改善。在28位2级小肠结肠炎患者中,有79%的患者完全消退,有11%的患者改善,有11%的患者没有改善。
黑色素瘤的辅助治疗
在CA184-029(NCT00636168)中接受YERVOY 10 mg / kg的患者中,76例患者(16%)发生3至5级免疫介导的小肠结肠炎,68例患者(14%)发生2级小肠结肠炎。7例患者(1.5%)出现肠穿孔,3例患者(0.6%)由于并发症而死亡[见不良反应(6.1) ]。
3至4级小肠结肠炎的发作中位时间为1.1个月(范围:1天至33.1个月),而2级小肠结肠炎的发作中位时间为1.1个月(范围为1天至20.6个月)。
接受全身性糖皮质激素治疗的3至4级小肠结肠炎患者共71例(95%)。中位治疗时间为4.7个月(最长52.3个月)。
在68例中度小肠结肠炎患者中,有51例(75%)接受了全身性皮质类固醇激素治疗,中位治疗时间为3.5个月(最长52.2个月)。非皮质类固醇的免疫抑制几乎完全由英夫利昔单抗组成,用于治疗36%的3至4级小肠结肠炎患者和15%的2级事件的患者。
在75例3至4级免疫介导的小肠结肠炎患者中,有86%的患者完全消退,有3%的患者达到1级好转,有11%的患者未好转。在68例2级小肠结肠炎患者中,有94%的患者完全消退,3%的患者达到1级好转,3%的患者未好转。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
免疫介导的结肠炎发生在10%(52/547)的RCC患者和7%(8/119)的CRC患者中。RCC患者的免疫介导性结肠炎发作的中位时间为1.7个月(范围:2天至19.2个月),而CRC患者的中位时间为2.4个月(范围:22天至5.2个月)。
免疫介导的结肠炎导致3.2%的RCC或CRC患者(n = 666)永久停用YERVOY和nivolumab,而3.9%的患者停用YERVOY和nivolumab [参见剂量和用法(2.5 ) ]。所有患有结肠炎的患者都需要全身性皮质类固醇激素,其中80%的患者接受了大剂量皮质类固醇激素(每天至少40 mg泼尼松当量),中位时间为21天(范围:1天至27个月)。大约23%的免疫介导性结肠炎患者需要在大剂量皮质类固醇激素中加入英夫利昔单抗。88%的患者发生了完全缓解。在用YERVOY重新启动nivolumab后,两名RCC患者复发了结肠炎。
5.2免疫介导的肝炎
YERVOY可能会发生免疫介导的肝炎,包括致命病例。
在每次服用YERVOY之前,监测肝功能测试(肝转氨酶和胆红素水平)并评估患者的肝毒性体征和症状。在具有肝毒性的患者中,排除感染或恶性病因,并增加对肝功能检查的监测频率,直至解决。
永久中止肝毒性3至4级的患者,并以1至2 mg / kg /天的泼尼松或同等剂量给予全身性皮质类固醇激素。当肝功能测试显示持续改善或恢复至基线时,开始皮质类固醇逐渐变细,并在1个月内逐渐缩小。在整个YERVOY的临床开发计划中,尽管有大剂量的皮质类固醇激素治疗,但仍患有持续性严重肝炎的患者接受了麦考酚酯治疗。对患有2级肝毒性的患者不给予YERVOY [请参阅剂量和用法(2.5) ]。
YERVOY作为单一代理
转移性黑色素瘤
在MDX010-20中接受YERVOY 3 mg / kg的患者,有严重,危及生命或致命的肝毒性(AST或ALT升高超过正常上限的5倍或总胆红素升高超过正常上限的3倍) ; 3至5级)发生在8例接受YERVOY治疗的患者中(占2%),在接受YERVOY治疗的患者中,致命肝衰竭的发生率为0.2%,住院率为0.4%。另有13名患者(2.5%)经历中度肝毒性,表现为肝功能检查异常(AST或ALT升高超过正常值或总胆红素升高上限的2.5倍至不超过5倍,但总胆红素升高不超过1.5倍但不超过高于正常上限的3倍; 2级)。并未在所有患者中确定潜在的病理,但在某些情况下包括免疫介导的肝炎。经活检证实为肝炎的患者人数不足以表征该事件的临床过程。
黑色素瘤的辅助治疗
在CA184-029中接受YERVOY 10 mg / kg的患者中,有51例患者(11%)发生了3至4级免疫介导的肝炎,有22例患者(5%)发生了中度2级免疫介导的肝炎。对6例3至4级肝炎患者进行的肝活检显示有中毒性或自身免疫性肝炎的证据。3至4级肝炎的中位发病时间为2.0个月(范围:1天至4.2个月),而2级肝炎的中位发病时间为1.4个月(范围:13天至6.5个月)。在51例3至4级免疫介导的肝炎患者中,有94%的患者完全消退,有4%的患者达到1级好转,有2%的患者未好转。在22位2级免疫介导的肝炎患者中,有91%的患者完全消退,而9%的患者无改善。
接受全身性皮质类固醇激素治疗的44例3至4级肝炎患者(占90%)。中位治疗时间为4.4个月(最长56.1个月)。用全身性皮质类固醇激素治疗了16例中度肝炎患者(73%)。中位治疗时间为2.6个月(最多41.4个月)。
与维拉非尼同时给药
在一项剂量寻找试验中,接受同时YERVOY(3 mg / kg)和vemurafenib(960 mg BID或720 mg BID)的10例患者中有6例发生转氨酶升高3级,总胆红素升高或不升高。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
免疫介导的肝炎发生在RCC患者的7%(38/547)和CRC患者的8%(10/119)。RCC患者的中位发病时间为2个月(范围:14天至26.8个月),而CRC患者的中位发病时间为2.2个月(范围:22天至10.5个月)。
免疫介导的肝炎导致3.6%的RCC或CRC患者(n = 666)永久停用YERVOY和nivolumab,而3.5%的患者则停用YERVOY和nivolumab [请参阅剂量和用法(2.5) ]。所有肝炎患者均需要全身性皮质类固醇激素治疗,其中94%的患者接受了大剂量皮质类固醇激素(每天至少40 mg泼尼松当量),中位时间为1个月(范围:1天至7个月)。大约19%的免疫介导性肝炎患者需要在大剂量皮质类固醇中添加麦考酚酸。83%的患者发生了完全消退。用YERVOY或单独使用nivolumab重新开始nivolumab后,没有患者再发肝炎。
5.3免疫介导的皮炎/皮肤不良反应
YERVOY可能发生免疫介导的皮炎,包括致命病例。
监测患者的皮炎体征和症状,例如皮疹和瘙痒。除非已确定其他病因,否则应将皮炎的体征或症状视为免疫介导的。
患有史蒂文斯-约翰逊综合征,中毒性表皮坏死症或皮疹并发全层皮肤溃疡或坏死,大疱或出血表现的患者,永久停用YERVOY。泼尼松或同等剂量的全身性皮质类固醇的剂量为1至2 mg / kg /天。当控制皮炎时,应至少在1个月内使皮质类固醇逐渐变细。中度至重度症状和体征的患者不使用YERVOY剂量[见剂量和用法(2.5) ]。
对于轻度至中度的皮炎,例如局部皮疹和瘙痒,请对症治疗。如果在1周内症状没有改善,则使用局部或全身性皮质类固醇。
YERVOY作为单一代理
转移性黑色素瘤
在MDX010-20中接受YERVOY 3 mg / kg的患者,发生严重,威胁生命或致命的免疫介导性皮炎(例如,史蒂文斯-约翰逊综合症,中毒性表皮坏死溶解或皮疹并发全层皮肤溃疡或坏死,大疱) ,或出血表现; 3至5级)发生在13例接受YERVOY治疗的患者中(2.5%)。一名患者(0.2%)由于毒性表皮坏死而死亡,另一名患者因严重的皮炎而需要住院治疗。有63例(12%)中度(2级)皮炎患者。
中度,重度或危及生命的免疫介导性皮炎发作的中位时间为22天,从开始YERVOY开始长达4.0个月。
7例接受YERVOY治疗的严重皮炎患者(54%)接受了大剂量皮质类固醇(中位数剂量60毫克泼尼松/天或同等剂量),治疗时间长达3.4个月,随后接受了皮质类固醇锥度治疗。在这7例患者中,有6例完全消退。解决时间最长为3.6个月。
在63例中度皮炎患者中,有25例(40%)接受全身性激素治疗(中位数为60毫克/天的泼尼松或同等剂量),平均治疗期为15天,其中7例(11%)仅接受局部皮质类固醇治疗, 31(49%)没有接受全身或局部皮质类固醇激素治疗。据报告有四十四名患者(70%)患有中度皮炎,可以完全消退,其中7名(11%)患者的病情好转至轻度(1级),而12名(19%)患者的病情没有改善。
黑色素瘤的辅助治疗
在CA184-029中接受YERVOY 10 mg / kg的患者中,有19例患者(4%)发生3至4级免疫介导的皮炎。有99例(21%)中度(2级)皮炎患者。3至4级皮炎的中位发病时间为14天(范围:5天至11.3个月),而2级皮炎的中位发病时间为11天(范围:1天至16.6个月)。
用全身性皮质类固醇激素治疗16例(3%至4级)皮炎患者(84%),中位时间为21天(最长49.2个月),从而在4.3个月的中位时间内(最长44.4个月)完全治愈了皮炎。 。在未接受全身或局部皮质类固醇治疗的3例患者中(16%),有2例(11%)完全消退,有1例改善为1级。
在99例2级皮炎患者中,有67例(68%)接受全身性皮质类固醇激素治疗,中间时间为2.6个月,其中16例(16%)仅接受局部皮质类固醇激素治疗,而16例(16%)未接受全身或局部皮质类固醇激素。77例患者(78%)完全消退,15例(15%)改善为轻度(1级),7例(7%)没有改善。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
免疫介导的皮疹发生在16%(90/547)的RCC患者和14%(17/119)的CRC患者中。RCC的中位发病时间为1.5个月(范围:1天至20.9个月),而CRC的中位发病时间为26天(范围:5天至9.8个月)。
免疫介导的皮疹导致0.5%的RCC或CRC患者(n = 666)永久性停药或停用YERVOY和nivolumab,2.6%的患者导致YERVOY和nivolumab停用[参见剂量和给药方法(2.5) ]。所有具有免疫介导性皮疹的患者都需要全身性皮质类固醇激素治疗,其中包括19%的患者接受大剂量皮质类固醇激素治疗(每天至少40 mg泼尼松当量),中位时间为22天(范围:1天至23个月)。66%的患者发生了完全缓解。免疫性皮疹复发的尼古鲁单抗患者约占3%(3/98)。
5.4免疫介导的神经病
YERVOY可能发生免疫介导的神经病,包括致命病例。
监测运动或感觉神经病的症状,例如单侧或双侧无力,感觉改变或感觉异常。在患有严重神经病(干扰日常活动)(例如格林-巴雷式综合征)的患者中,永久停用YERVOY。进行适当的医学干预以应对严重的神经病。对于严重的神经病,考虑以1至2 mg / kg /天的泼尼松剂量或与之等效的剂量开始全身性皮质类固醇激素治疗。中度神经病(不干扰日常活动)的患者不使用YERVOY剂量[见剂量和用法(2.5) ]。
YERVOY作为单一代理
转移性黑色素瘤
在MDX010-20中接受YERVOY 3 mg / kg的患者中,报告了1例致命的格林-巴利综合征和1例严重的(3级)周围运动神经病。在YERVOY的整个临床开发计划中,已经报告了重症肌无力和格林-巴利综合征的其他病例。
黑色素瘤的辅助治疗
在CA184-029中接受YERVOY 10 mg / kg的患者中,8例患者(2%)发生了3至5级免疫介导的神经病。唯一的死亡是由于格林-巴利综合征的并发症[见不良反应(6.1) ]。1例患者发生了中度2级免疫介导的神经病变(0.2%)。
9名2至5级免疫介导的神经病患者的发病时间为1.4至27.4个月。所有8例3至5级神经病变的患者均接受了全身性糖皮质激素治疗(范围:3天至38.3个月),其中3例也接受了他克莫司治疗。8例3至5级免疫介导的神经病患者中有4例完全消退,1例改善为1级,3例未改善。患有2级免疫介导的神经病的单例患者无需使用皮质类固醇即可完全缓解。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
在547例RCC患者中,有3例3级感觉异常/感觉不足。
5.5免疫介导的内分泌病变
YERVOY可能会发生免疫介导的内分泌病变,包括危及生命的病例。
监测患者的垂体炎,肾上腺功能不全(包括肾上腺危机)以及甲状腺功能亢进或甲状腺功能减退的临床体征和症状。患者可能会出现疲劳,头痛,精神状态改变,腹痛,异常的排便习惯和低血压,或可能类似于其他原因(例如脑转移或潜在疾病)的非特异性症状。除非已发现其他病因,否则应将内分泌病的体征或症状视为免疫介导的。
在治疗开始时,每次给药前以及根据症状根据临床指示监测临床化学,促肾上腺皮质激素(ACTH)水平和甲状腺功能测试。在少数患者中,通过影像学检查可通过垂体腺增大诊断出垂体不足。
对有症状的患者不服用YERVOY,并考虑转诊给内分泌科医生。以1到2 mg / kg /天的泼尼松或同等剂量开始全身性皮质类固醇激素治疗,并开始适当的激素替代疗法[见剂量和用法(2.5) ]。
YERVOY作为单一代理
转移性黑色素瘤
在MDX010-20中接受3毫克/千克YERVOY的患者中,有9例接受YERVOY治疗的患者发生了严重至危及生命的免疫介导的内分泌病变(需要住院,紧急医疗干预或干扰日常生活; 3至4级) (1.8%)。9例患者均患有垂体功能低下,另一些伴有内分泌病变,如肾上腺功能不全,性腺功能低下和甲状腺功能减退。9例患者中有6例因严重内分泌病变而住院。中度内分泌病(需要激素替代或医学干预; 2级)发生在12例患者(2.3%)中,由甲状腺功能减退,肾上腺功能不全,垂体功能低下以及甲亢和库欣综合征各1例组成。中度至重度免疫介导的内分泌病发作的中位时间为2。
在21例中度至危及生命的内分泌病患者中,有17例需要长期激素替代治疗,其中最常见的是肾上腺激素(n = 10)和甲状腺激素(n = 13)。
黑色素瘤的辅助治疗
在CA184-029中接受YERVOY 10 mg / kg的患者中,39例患者(8%)发生了3至4级免疫介导的内分泌病,93例患者(20%)发生了2级免疫介导的内分泌病。在39例3至4级免疫介导的内分泌病患者中,有35例患有垂体机能减退(伴有一种或多种继发性内分泌病,例如肾上腺功能不全,性腺功能减退和甲状腺功能低下),其中3例患有甲状腺功能亢进,1例患有原发性甲状腺功能减退。3至4级免疫介导的内分泌病发作的中位时间为2.2个月(范围:2天至8个月)。39例患者中有27例(69%)因免疫介导的内分泌病而住院,据报道有4例(10%)可以消退。
在93例2级免疫介导的内分泌病患者中,有74例患有原发性垂体机能减退(与一种或多种继发性内分泌病相关,例如肾上腺功能不全,性腺功能低下和甲状腺功能减退),9例原发性甲状腺功能减退,3例甲状腺功能亢进,3例甲状腺功能低下-或甲亢,2患有性腺机能减退,1既有甲状腺功能亢进又有垂体机能减退,1受试者患有Graves眼病。2级免疫介导的内分泌病发作的中位时间为2.1个月(范围:9天至19.3个月),据报道有20%的患者可以解决。
124例患者接受了全身性皮质类固醇激素的免疫抑制和/或肾上腺激素替代,以治疗2至4级免疫介导的内分泌病。其中42(34%)人能够停用皮质类固醇。73例患者接受了甲状腺激素以治疗2至4级免疫介导的甲状腺功能减退症。其中,有14名患者(19%)可以停止甲状腺替代治疗。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
垂体炎。垂体增生发生在RCC患者的4.6%(25/547)和CRC患者的3.4%(4/119)。RCC患者的中位发病时间为2.8个月(范围:1.3个月至7.3个月),CRC患者的中位发病时间为3.7个月(范围:2.8至5.5个月)。
垂体炎分别导致1.2%和2.6%的RCC或CRC患者(n = 666)永久终止或停用YERVOY和nivolumab [见剂量和给药方法(2.5) ]。大约72%的垂体炎患者接受了激素替代治疗,55%的患者接受了大剂量皮质类固醇(每天至少40 mg泼尼松当量),中位时间为13天(范围:1天至1.6个月)。
肾上腺功能不全。肾上腺功能不全的发生率分别为7%(41/547)的RCC患者和5.9%(7/119)的CRC患者。RCC的中位发病时间为3.4个月(范围:2.0个月至22.3个月),CRC的中位发病时间为3.7个月(范围:2.5至13.4个月)。
肾上腺功能不全导致1.2%的RCC或CRC患者(n = 666)永久停用YERVOY和nivolumab,2.6%的患者停用YERVOY和nivolumab [见剂量和用法(2.5) ]。约94%的肾上腺功能不全患者接受了激素替代治疗,而27%的患者接受了大剂量皮质类固醇(每天至少40 mg泼尼松当量),中位时间为12天(范围:2天至5.6个月)。
甲状腺功能低下和甲状腺功能亢进。甲状腺功能减退或甲状腺炎导致甲状腺功能减退的患者中,RCC患者为22%(119/547),CRC患者为15%(18/119)。RCC患者的中位发病时间为2.2个月(范围:1天至21.4个月),而CRC患者的中位发病时间为2.3个月(范围:22天至9.8个月)。在137例发生甲状腺功能减退的RCC或CRC患者中,约81%的RCC患者和78%的CRC患者接受了左甲状腺素。
甲状腺功能亢进发生在12%(66/547)的RCC患者和12%(14/119)的CRC患者中。RCC的中位发病时间为1.4个月(范围:6天至14.2个月),CRC的中位发病时间为1.1个月(范围:21天至5.4个月)。在80例发展为甲状腺功能亢进的RCC或CRC患者中,约15%的患者接受了methimazole,2%的患者接受了carbimazole。
1型糖尿病。2.7%(15/547)的RCC患者患有糖尿病。发作的中位时间为3.2个月(范围:19天至16.8个月)。YERVOY和nivolumab均在33%的患者中被停用,而在20%的糖尿病患者中均被永久停用[参见剂量和给药方法(2.5) ]。
5.6免疫介导的肺炎
尼古鲁单抗联合YERVOY可发生免疫介导的肺炎,包括致命病例。监视患者影像学检查的体征和肺炎的症状。对于中度(2级)或更严重(3-4级)的肺炎,以1至2 mg / kg /天泼尼松当量的剂量给予皮质类固醇激素,然后逐渐减量。中度至重度体征和症状的患者应停用YERVOY剂量。永久终止YERVOY治疗危及生命(4级)的肺炎[见剂量和用法(2.5) ]。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
免疫介导的肺炎发生在4.4%(24/547)的RCC患者和1.7%(2/119)的CRC患者中。RCC患者发生免疫介导性肺炎的中位时间为2.6个月(范围:8天至9.2个月),CRC患者为1.9个月(范围:27天至3个月)。
免疫介导的肺炎导致1.8%的RCC或CRC患者(n = 666)永久终止YERVOY和nivolumab,1.7%的患者停用YERVOY和nivolumab [请参阅剂量和用法(2.5) ]。所有患有肺炎的患者都需要全身性皮质类固醇激素治疗,其中92%的患者接受了大剂量皮质类固醇激素治疗(每天至少40 mg泼尼松当量),中位时间为19天(范围:4天至3.2个月)。大约8%需要在大剂量皮质类固醇中添加英夫利昔单抗。肺炎的完全解决在81%的患者中发生。
5.7免疫介导的肾炎和肾功能不全
尼罗单抗联合YERVOY可发生免疫介导的肾炎。在治疗之前和治疗期间定期监测患者的血清肌酐水平。给予1至2 mg / kg /天泼尼松当量的剂量的皮质类固醇激素,然后逐渐减量使用皮质类固醇激素(第4级),增加血清肌酐。中度(2级)或严重(3级)血清肌酐增加时,以0.5至1 mg / kg /天泼尼松当量的剂量给予皮质类固醇,如果恶化或没有改善,将皮质类固醇剂量增加至1-2 mg / kg /天泼尼松当量。中度至重度体征和症状的患者应停用YERVOY剂量。永久终止YERVOY以危及生命(4级)血清肌酐水平升高[参见剂量和用法(2.5) ]。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
免疫介导的肾炎和肾功能不全的发生率分别为RCC患者的4.6%(25/547)和CRC患者的1.7%(2/119)。在这27例患者中,中位发作时间为3个月(范围:1天至13.2个月)。
免疫介导的肾炎和肾功能不全导致RCC或CRC(n = 666)的患者中有1.2%的YERVOY和nivolumab永久性停药,而RCC或CRC的患者中2.3%的患者有nivolumab和YERVOY的停药[参见剂量和给药方法( 2.5) ]。约有78%的免疫介导性肾炎和肾功能不全患者接受高剂量皮质类固醇激素(每天至少40 mg泼尼松当量),中位时间为17天(范围:1天至6个月)。63%的患者发生了完全消退。
5.8免疫介导性脑炎
免疫介导的脑炎可以与YERVOY一起发生。对具有神经系统症状的患者的评估可能包括但不限于咨询神经科医生,脑部MRI和腰椎穿刺。
在新发中度至重度神经系统症状或症状的患者中不接受YERVOY治疗,并评估排除中度至重度神经系统恶化的传染病或其他原因。如果排除其他病因,对于免疫介导的脑炎患者,以1至2 mg / kg /天泼尼松当量的剂量给予皮质类固醇激素,然后进行皮质类固醇锥度治疗。对于免疫介导的脑炎,永久停用YERVOY [请参阅剂量和给药方法(2.5) ]。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
在开始YERVOY后约4个月,一名RCC患者(0.2%)发生脑炎,在开始YERVOY 15天后发生CRC的一名患者(0.8%)。CRC患者需要英夫利昔单抗和大剂量皮质类固醇(每天至少40 mg泼尼松当量)。
5.9输液反应
尼伏鲁单抗与YERVOY可能发生严重的输注反应。有严重或危及生命的输注反应的患者中止使用YERVOY。中度或中度输注反应患者的输注速度中断或减慢[见剂量和用法(2.5) ]。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
输注相关反应发生在5.1%(28/547)的RCC患者和4.2%(5/119)的CRC患者中。
5.10其他免疫介导的不良反应
YERVOY作为单一代理
对于临床意义重大或严重的免疫介导的不良反应,请永久终止YERVOY。以1到2 mg / kg /天的泼尼松剂量或等效剂量开始全身性皮质类固醇激素治疗,以引起严重的免疫介导的不良反应。
监测患者的眼毒性体征或症状,包括视力模糊和视力下降。免疫介导的眼毒性可能与视网膜脱离或永久性视力丧失有关。给患有葡萄膜炎,虹膜炎或巩膜炎的患者服用皮质类固醇滴眼液。对于对局部免疫抑制疗法无反应的免疫介导的眼部疾病,永久停用YERVOY [请参阅剂量和给药方法(2.5) ]。如果葡萄膜炎与其他免疫介导的不良反应同时发生,请考虑接受Vogt-Koyanagi-Harada样综合征,该综合征已在接受YERVOY的患者中观察到,可能需要全身性类固醇治疗以减少永久性视力丧失的风险。
在异基因造血干细胞移植(HSCT)之前或之后接受CTLA-4受体阻断抗体的患者可能发生致命或严重的移植物抗宿主病(GVHD)。密切跟踪患者以获取GVHD的证据,并立即进行干预。[参见不良反应(6.2)。]考虑异基因HSCT后使用CTLA-4受体阻断抗体治疗的益处与风险。
转移性黑色素瘤
在MDX010-20中,在不到1%的YERVOY治疗患者中观察到以下临床上重要的免疫介导的不良反应:血细胞减少症,肾炎,肺炎,脑膜炎,心包炎,葡萄膜炎和虹膜炎。
黑色素瘤的辅助治疗
在CA184-029中,除非另有说明,在不到1%的YERVOY治疗患者中观察到以下临床上重要的免疫介导的不良反应:血细胞减少症,嗜酸性粒细胞增多症(2.1%),胰腺炎(1.3%),脑膜炎,肺炎,结节病,心包炎,葡萄膜炎和致命性心肌炎[请参阅不良反应(6.1) ]。
其他临床经验
在以0.1至20 mg / kg(n = 2478)的剂量施用YERVOY的21项剂量范围试验中,除非另有说明,还报告了以下可能的免疫介导的不良反应,发生率不到1%:血管病,颞动脉炎,血管炎,风湿性多肌痛,结膜炎,睑缘炎,巩膜炎,巩膜炎,虹膜炎,白细胞碎裂性血管炎,多形性红斑,牛皮癣,关节炎,自身免疫性甲状腺炎,神经感觉性听觉过敏,自身免疫性中枢神经病(脑炎),肌炎,肌炎,多发性肌炎,肾炎。
YERVOY 1毫克/公斤,尼古拉单抗3毫克/公斤
YERVOY可以引起其他临床上重要的和潜在致命的免疫介导的不良反应。终止YERVOY治疗后可能发生免疫介导的不良反应。对于任何怀疑的免疫介导的不良反应,请排除其他原因。根据不良反应的严重程度,永久终止或停用YERVOY,给予大剂量皮质类固醇,并在适当的情况下开始激素替代治疗。改善至1级或以下后,开始逐渐降低皮质类固醇激素水平,并持续降低锥度至少1个月。根据事件的严重程度,考虑在完成皮质类固醇锥度治疗后重新开始YERVOY。
在YERVOY尼伏鲁单抗治疗或单药尼伏鲁单抗治疗的整个临床试验中,以下不到1.0%的患者发生以下临床上明显的免疫介导的不良反应,其中一些具有致命后果:心肌炎,横纹肌溶解,肌炎,葡萄膜炎,虹膜炎,胰腺炎,面部和外展神经麻痹,脱髓鞘,风湿性多肌痛,自身免疫性神经病,格林-巴雷综合征,垂体机能减退,全身性炎症反应综合征,胃炎,十二指肠炎,结节病,组织细胞坏死性淋巴结炎,气管淋巴结炎,气管功能性淋巴结炎(Kikuchi淋巴结炎)再生障碍性贫血,心包炎和肌无力综合征。
5.11胚胎-胎儿毒性
根据其作用机理和动物研究数据,施予孕妇时,YERVOY可能引起胎儿伤害。在动物生殖研究中,从器官发生开始到分娩开始向食蟹猕猴施用依匹木单抗会导致流产,死产,早产(相应降低出生体重)的发生率更高,并且以剂量相关的方式导致婴儿死亡的发生率也更高。依匹莫单抗的作用在妊娠中期和中期可能更大。建议孕妇注意胎儿的潜在危险。建议有生殖潜力的女性在使用含YERVOY的治疗方案期间以及最后一次使用YERVOY后3个月内使用有效的避孕方法[请参阅使用在特殊人群(8.1,8.3) ]。
5.12与Nivolumab联用时的相关风险
当YERVOY与nivolumab联合使用时,请参阅nivolumab处方信息,以获得适用于联合使用的其他风险信息。
6不良反应
标签的其他部分将详细讨论以下不良反应。
• 免疫介导的小肠结肠炎/结肠炎[请参阅警告和注意事项(5.1) ]。
• 免疫介导的肝炎[参见警告和注意事项(5.2) ]。
• 免疫介导的皮炎/皮肤不良反应[请参阅警告和注意事项(5.3) ]。
• 免疫介导的神经病[请参阅警告和注意事项(5.4) ]。
• 免疫介导的内分泌病[请参阅警告和注意事项(5.5) ]。
• 免疫介导的肺炎[请参阅警告和注意事项(5.6) ]。
• 免疫介导的肾炎和肾功能不全[见警告和注意事项(5.7) ]。
• 免疫介导的脑炎[请参阅警告和注意事项(5.8) ]。
• 输液反应[请参阅警告和注意事项(5.9) ]。
• 其他免疫介导的不良反应[请参阅警告和注意事项(5.10) ]。
• 胚胎胎儿毒性[见警告和注意事项(5.11) ]。
在MDX010-20中因不可切除或转移性黑素瘤接受YERVOY 3 mg / kg的患者中,接受单药治疗的患者中有15%接受gp100肽疫苗联合治疗的患者中有12%发生了3至5级免疫介导的反应。在CA184-029中接受YERVOY 10 mg / kg的黑色素瘤辅助治疗的患者中,有41%的患者经历了3至5级免疫介导的反应。
6.1临床试验经验
由于临床试验是在广泛不同的条件下进行的,因此观察到的不良反应发生率无法直接与其他临床试验中的发生率进行比较,也无法直接与同类疗法的经验进行比较,并且可能无法反映临床实践中观察到的发生率。
下述数据反映了MDX010-20中单一药物暴露于YERVOY 3 mg / kg的情况,这是一项针对不可切除或转移性黑色素瘤患者的随机试验;在CA184-029中以单药的剂量达到YERVOY 10 mg / kg,这是一项针对IIIA期(> 1 mm淋巴结转移),IIIB和IIIC期(无转移性转移)皮肤黑色素瘤切除患者的随机试验;在两项试验中,与nivolumab联合给予YERVOY 1 mg / kg:一项先前未接受治疗的晚期肾细胞癌患者的随机试验,CHECKMATE-214(NCT02231749),以及开放标签的CHECKMATE-142(NCT02060188) ,先前接受过MSI-H或dMMR转移性结直肠癌治疗的患者的多中心,非随机,多平行平行队列研究。
在以MDX010-20和CA184-029治疗的982例患者中,以及在以0.1至20 mg / kg的剂量给予YERVOY的21项剂量范围试验(n = 2478)中,对临床上显着的不良反应进行了评估[请参阅警告和注意事项( 5.6) ]。
不可切除或转移性黑色素瘤
YERVOY的安全性在MDX010-20中进行了评估,MDX010-20是一项随机,双盲临床试验,其中643例先前接受治疗的不可切除或转移性黑色素瘤患者接受了4剂YERVOY 3 mg / kg静脉输注,作为单一药物(n = 131),使用研究性gp100肽疫苗(gp100)(n = 380)或gp100肽疫苗作为单药(n = 132)的YERVOY [请参阅临床研究(14.1) ]。试验中的患者接受了4剂的中位数(范围:1到4剂)。
MDX010-20排除了患有活动性自身免疫病或接受全身免疫抑制的器官移植患者。
试验人群特征为:中位年龄57岁(范围:19至90岁),男性59%,白人94%,基线ECOG表现状态0(56%)。
10%的患者因不良反应而停止使用YERVOY。
表2列出了来自MDX010-20的某些不良反应,这些不良反应发生在含YERVOY的组中至少5%的患者中,对于所有等级的事件,其发生率比对照组gp100的组增加了至少5%,且发生率至少为1%超过对照组的3至5级事件。
表2:MDX010-20中的某些不良反应
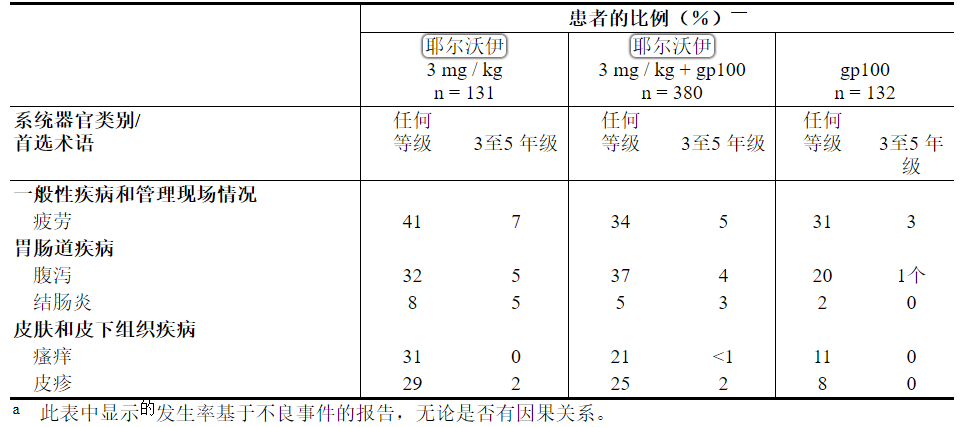
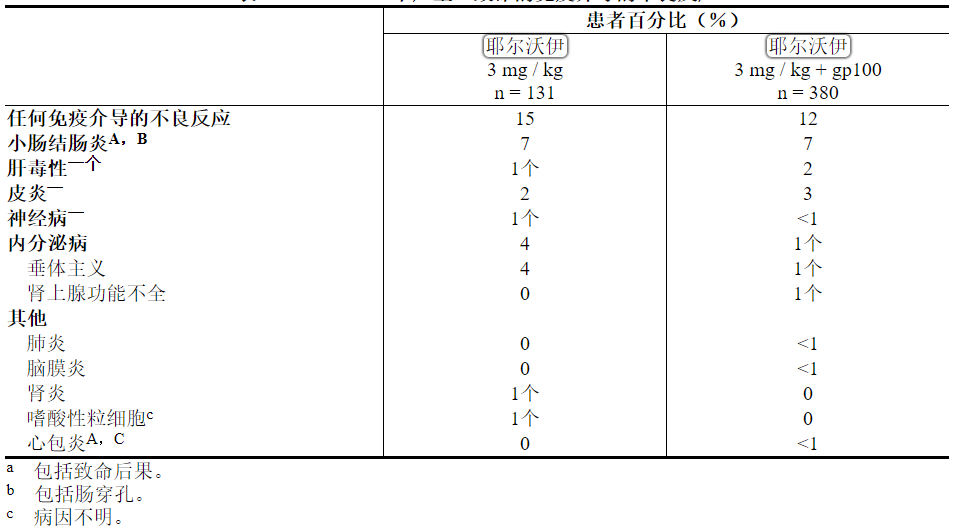
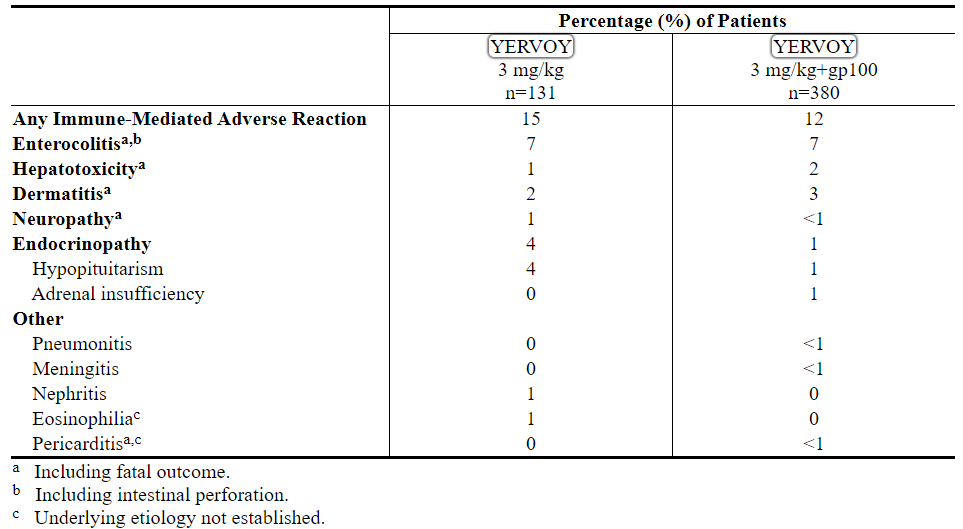
表3列出了来自MDX010-20的严重,威胁生命或致命的免疫介导的不良反应的每患者发生率。
表3:MDX010-20中严重至致命的免疫介导的不良反应
黑色素瘤的辅助治疗
在CA184-029(一项随机(1:1),双盲,安慰剂对照试验)中评估了YERVOY的安全性,该试验中945例切除了IIIA期(淋巴结受累> 1 mm),IIIB和IIIC期(无转移中)皮肤黑素瘤接受YERVOY 10 mg / kg(n = 471)或安慰剂(n = 474)静脉输注,每3周给药4剂,随后从第24周起每12周给药10 mg / kg最多3年[参见临床研究(14.2) ]。在该试验中,36%的患者接受YERVOY的时间超过6个月,而26%的患者接受YERVOY的时间超过1年。该试验中接受YERVOY治疗的患者平均接受了4剂(范围:1至16)。
CA184-029排除了先前接受过黑色素瘤全身性治疗,自身免疫性疾病,需要全身性免疫抑制或对乙型肝炎,丙型肝炎或HIV阳性的患者。
试验人群特征为:中位年龄51岁(范围:18至84岁),男性62%,白人99%,基线ECOG表现状态0(94%)。
在52%的患者中因不良反应而停止使用YERVOY。
表4列出了从CA184-029中选择的不良反应,这些不良反应发生在至少5%的YERVOY治疗患者中,并且在所有级别的事件中,与安慰剂组相比,发生率至少增加了5%。
表4:CA184-029中的不良反应
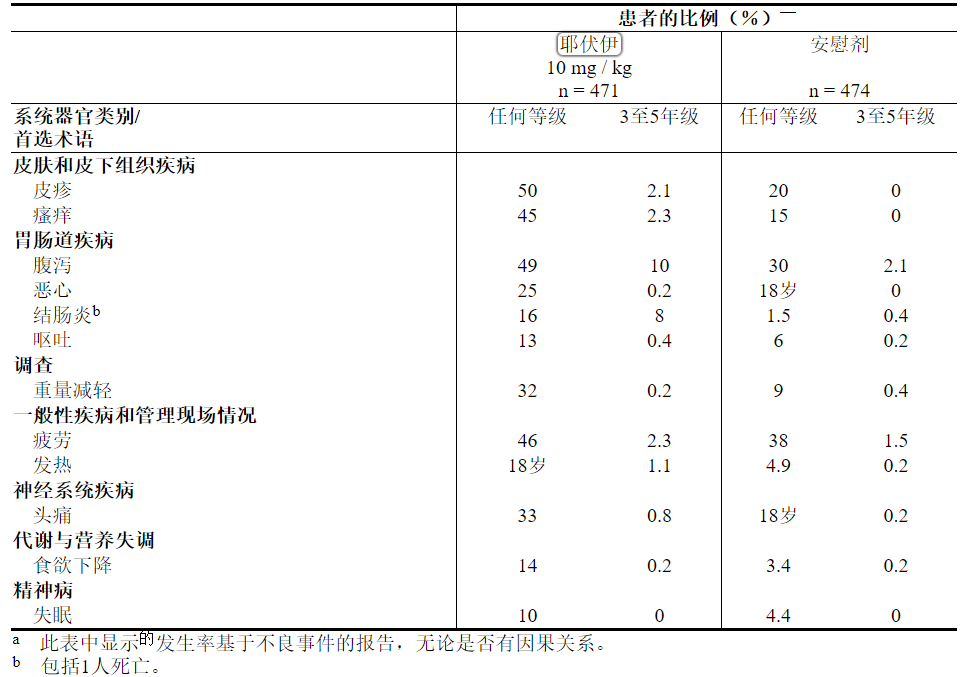
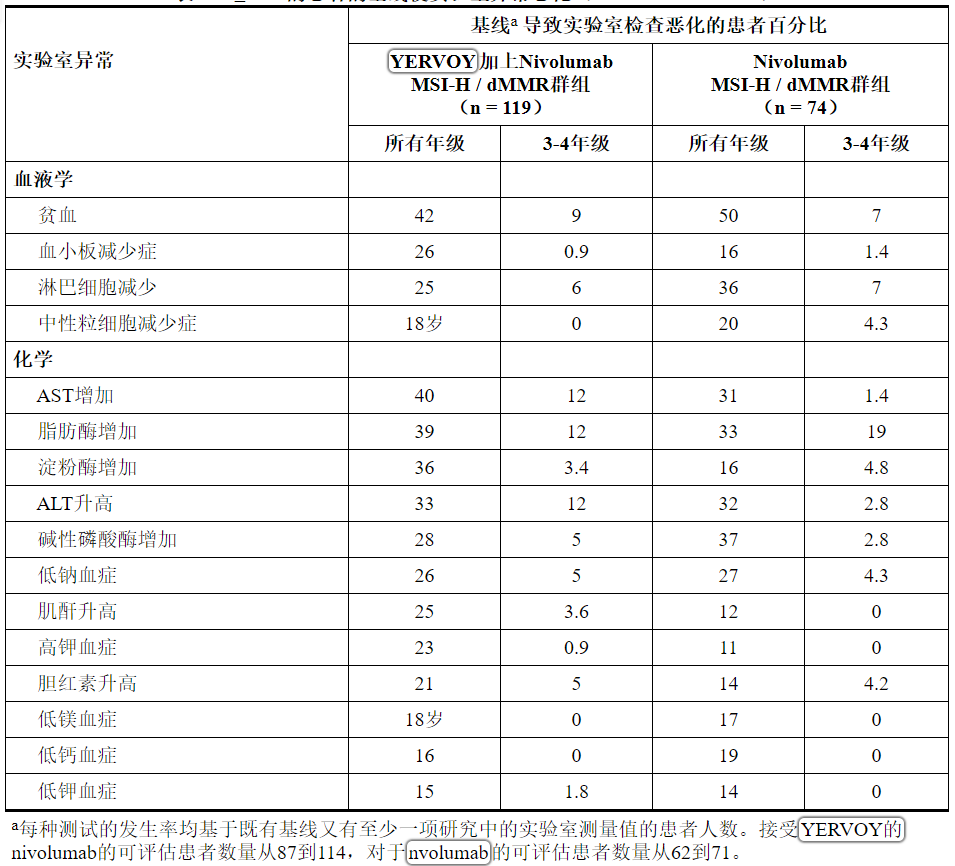
表5列出了从CA184-029中选择的实验室异常,这些异常发生在至少10%的YERVOY治疗患者中,发生率高于安慰剂。
表5:≥10%接受YERVOY治疗的患者的基线异常使实验室异常恶化(CA184-029)a
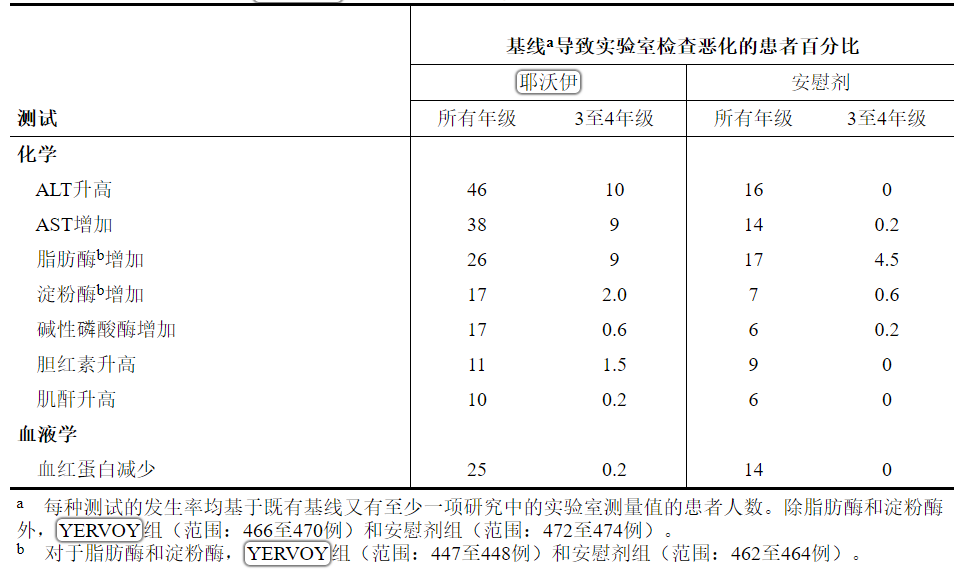
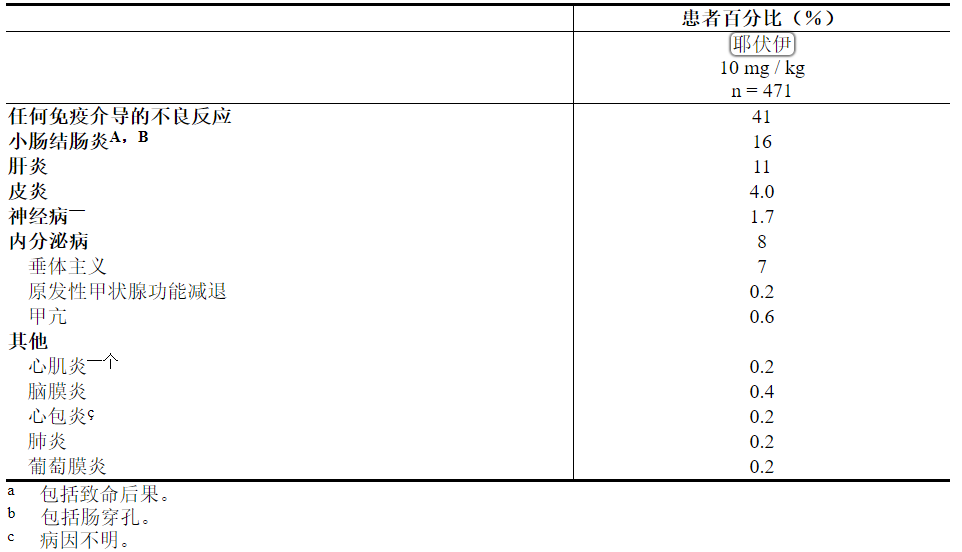
表6列出了CA184-029中每例患者发生的严重,威胁生命或致命的免疫介导的不良反应的发生率。
表6:CA184-029中严重至致命的免疫介导的不良反应
其他临床经验
在所有使用0.3至10 mg / kg的YERVOY剂量的临床研究中,还报告了以下不良反应(除非另有说明,发生率小于1%):荨麻疹(2%),大肠溃疡,食道炎,急性呼吸窘迫综合征,肾功能衰竭和输液反应。
先前未经治疗的肾细胞癌
在CHECKMATE-214中评估了以1毫克/千克的YERVOY施用3毫克/千克的nivolumab的安全性,这是一项随机开放标签试验,其中1082例先前未接受治疗的晚期RCC患者接受3毫克/千克的nivolumab联合1毫克的YERVOY每3周/ kg服用4剂,然后每2周以3 mg / kg剂量进行nivolumab单药治疗(n = 547),或者每个周期每天口服50 mg舒尼替尼治疗4周,然后每2周停用2周(n = 535)[请参阅临床研究(14.3) ]。接受nivolumab + YERVOY治疗的患者的中位治疗时间为7.9个月(范围:1天至21.4+个月),接受舒尼替尼治疗的患者的中位治疗时间为7.8个月(范围:1天至20.2+个月)。在该试验中,尼古鲁单抗+ YERVOY组中有57%的患者接受了超过6个月的治疗,而38%的患者接受了超过1年的治疗。
31%的nivolumab加YERVOY患者和21%的舒尼替尼患者因不良反应而停止研究治疗。接受nivolumab联合YERVOY的患者中有54%(54%),接受舒尼替尼的患者中有43%因不良反应而延误药物治疗。在舒尼替尼组中,有53%的患者需要降低剂量;nivolumab + YERVOY治疗组不允许降低剂量。接受nivolumab加YERVOY的患者中有59%发生严重不良反应,接受舒尼替尼的患者中有43%发生严重不良反应。在至少2%的接受nivolumab加YERVOY治疗的患者中,最常见的严重不良反应是腹泻,发热,肺炎,肺炎,垂体炎,急性肾损伤,呼吸困难,肾上腺功能不全和结肠炎;在接受舒尼替尼治疗的患者中,他们患有肺炎,
最常见的不良反应(据报道至少有20%的nivolumab加上YERVOY治疗的患者)为疲劳,皮疹,腹泻,肌肉骨骼疼痛,瘙痒,恶心,咳嗽,发热,关节痛,呕吐,呼吸困难和食欲下降。表7总结了超过15%的nivolumab加YERVOY治疗的患者发生的不良反应。
表7:超过15%的接受Nivolumab加YERVOY的患者出现1-4级不良反应(CHECKMATE-214)

与基线相比,≥30%的nivolumab加YERVOY治疗的患者最常见的实验室异常较基线恶化,包括脂肪酶升高,贫血,肌酐升高,ALT升高,AST升高,低钠血症,淀粉酶升高和淋巴细胞减少。表8总结了超过15%的nivolumab加YERVOY治疗的患者发生的实验室异常。
表8:超过15%的Nivolumab联合YERVOY患者的基线发生的1-4级实验室值恶化(CHECKMATE-214)

此外,与舒尼替尼组相比,在尼古卢单抗+ YERVOY组中,基线时TSH小于或等于ULN的患者中,发生治疗前TSH升高高于ULN的患者比例较低(31%和61% %, 分别)。
先前治疗过的MSI-H或dMMR转移性结直肠癌
在开放式,多中心,非随机,多队列研究中,CHECKMATE-142对YERVOY的安全性进行了评估。在CHECKMATE-142中,单臂队列研究中有119名先前接受过MSI-H或dMMR mCRC治疗的患者接受了YERVOY联合nivolumab治疗。在CHECKMATE-142下的另一组单臂队列中,有74名mCRC患者接受了nivolumab单药治疗。两个队列中的所有患者均已接受过基于氟尿嘧啶的化学疗法治疗转移性疾病。在YERVOY和nivolumab队列中,有69%的患者接受过氟嘧啶,奥沙利铂和伊立替康的事先治疗,而29%的患者接受了抗EGFR抗体。
YERVOY联合nivolumab队列的患者在每个21天周期的第1天接受4剂量的YERVOY 1 mg / kg和nivolumab 3 mg / kg,然后每2周接受3 mg / kg nivolumab,直到疾病进展或出现不可接受的毒性。在nivolumab单药研究组中,患者每3周接受3 mg / kg nivolumab,直到疾病进展或出现不可接受的毒性[见临床研究(14.4) ]。
YERVOY的中位暴露时间为2.1个月。在接受YERVOY治疗的患者中,有47%发生了严重的不良反应。在至少2%的患者中,最常见的严重不良反应为结肠炎/腹泻,肝病,腹痛,急性肾损伤,发热和脱水。最常见的不良反应(报告于YERVOY治疗的患者中至少20%)是疲劳,腹泻,发热,肌肉骨骼疼痛,腹痛,瘙痒,恶心,皮疹,食欲下降和呕吐。
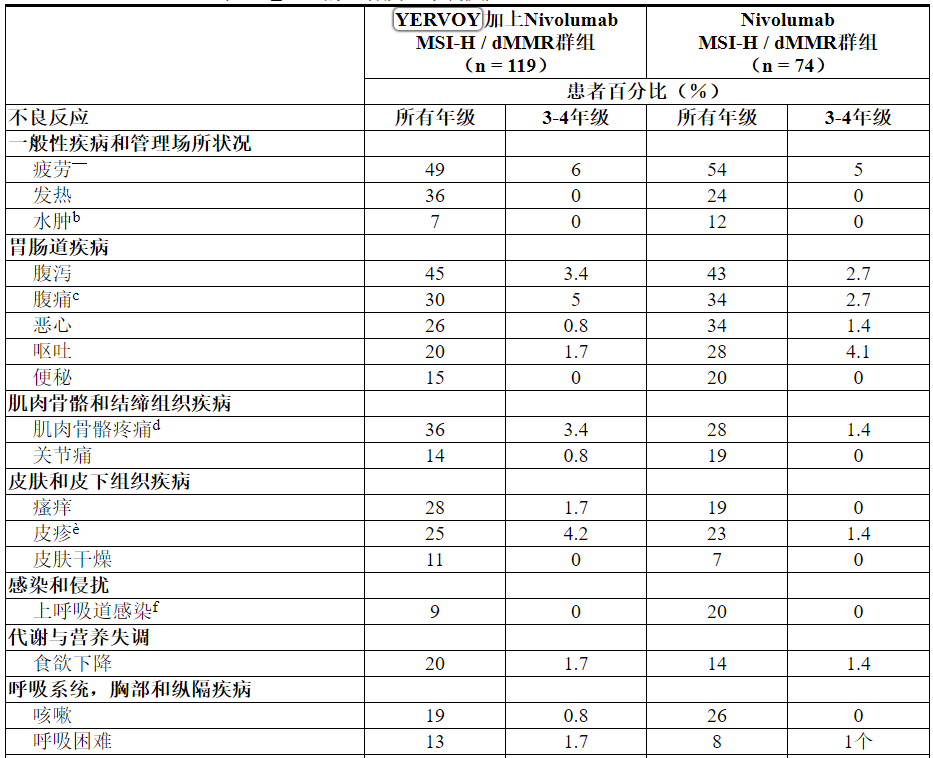
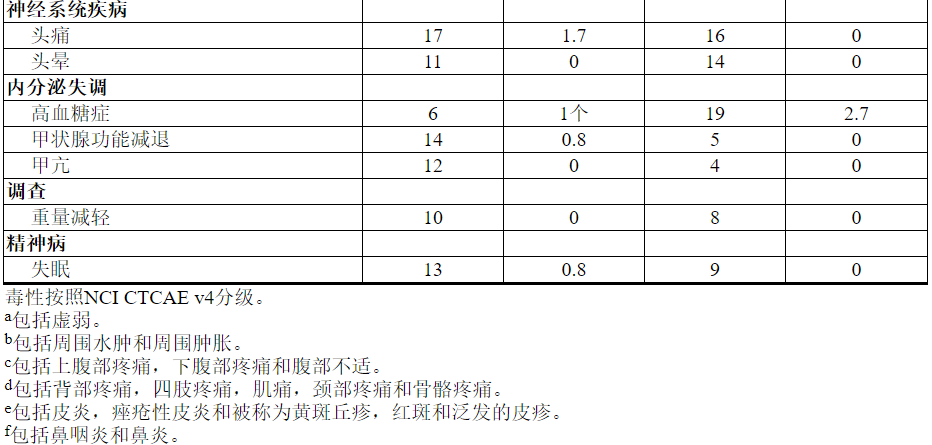
表9总结了超过10%的接受YERVOY的患者发生的不良反应。表10总结了接受YERVOY的患者中超过10%的实验室检查结果较基线水平有所恶化。基于CHECKMATE-142的设计,以下总结的数据不能用于识别两个队列之间任何不良反应的统计学显着差异。
表9:≥10%的患者发生不良反应(CHECKMATE-142)
在CHECKMATE-142中接受YERVOY治疗的不到10%的其他临床重要不良反应为脑炎(0.8%),坏死性肌炎(0.8%)和葡萄膜炎(0.8%)。
表10:≥10%的患者的基线使实验室异常恶化(CHECKMATE-142)
6.2售后经验
在YERVOY的批准后使用过程中,发现了以下不良反应。由于这些反应是从不确定大小的人群中自愿报告的,因此并非总是能够可靠地估计其发生频率或建立与药物暴露的因果关系。
免疫系统疾病:移植物抗宿主病
皮肤和皮下组织疾病:具有嗜酸性粒细胞增多和全身症状(DRESS综合征)的药物反应
6.3免疫原性
与所有治疗性蛋白质一样,具有免疫原性的潜力。抗体形成的检测高度依赖于测定的灵敏度和特异性。另外,在测定中观察到的抗体(包括中和抗体)阳性的发生率可能受到几个因素的影响,包括测定方法,样品处理,样品收集的时间,伴随用药和基础疾病。由于这些原因,将下述研究中的伊匹木单抗抗体的发生率与其他研究或其他产品中抗体的发生率进行比较可能会产生误导。
1024名可评估患者患有不可切除或转移性黑素瘤十一(1.1%)测试的正面为治疗后出现的结合对的抗体易普利姆玛在电化学发光(ECL)的测定(TE-ADAS)。该测定在存在ipilimumab的情况下在检测抗ipilimumab抗体方面有很大的局限性。144例接受伊立木单抗治疗的患者中有7(4.9%)和156例接受安慰剂治疗黑色素瘤的接受安慰剂的患者中有7(4.5%)使用改善了药物耐受性的ECL分析对TE-ADAs呈阳性反应。没有患者的中和抗体测试呈阳性。TE-ADA呈阳性的患者未发生与输注相关的反应。
的499例患者可评价抗易普利姆玛在CHECKMATE-214和CHECKMATE-142,27(5.4%)的抗体呈阳性抗易普利姆玛抗体; 没有患者有抗ipilimumab中和抗体。没有证据显示抗伊利木单抗抗体的患者对YERVOY的输注反应发生率增加。在CHECKMATE-214和CHECKMATE-142试验的503例可评估抗nivolumab抗体的患者中,126例(25%)的抗nivolumab抗体呈阳性,3例(0.6%)的中性抗nivolumab抗体呈阳性。
7药物相互作用
YERVOY尚未进行正式的药代动力学药物相互作用研究。
8在特定人群中的使用
8.1怀孕
风险摘要
根据动物研究的数据及其作用机理,YERVOY对孕妇给药可引起胎儿伤害[见临床药理学(12.1) ]。在动物生殖研究中,从器官发生开始到分娩开始向食蟹猕猴施用依匹木单抗会导致更高的流产,死产,早产(相应降低出生体重)的发生率,并以剂量相关的方式增加婴儿死亡率的发生率(见数据)。依匹莫单抗的作用在妊娠中期和中期可能更大。已知人类IgG1可以穿过胎盘屏障和ipilimumab是IgG1;因此,ipilimumab有潜力从母亲传播给发育中的胎儿。没有足够的孕妇YERVOY暴露数据。建议孕妇注意胎儿的潜在危险。
在美国普通人群中,临床公认的怀孕中主要先天缺陷和流产的估计背景风险分别为2%至4%和15%至20%。
已经建立了怀孕安全性监视研究,以收集有关接受YERVOY的女性怀孕的信息。鼓励医疗保健提供者招募患者或致电1-844-593-7869让他们的患者直接招募。
数据
动物资料
在胚胎-胎儿和围出生后发育的组合研究中,怀孕食蟹猴接受易普利姆玛每3周从器官发生的发作在第一三个月通过分娩。在怀孕的前两个月中未发现与治疗有关的生殖不良影响。从孕晚期开始,以3 mg / kg的剂量暴露ipilimumab的剂量约为人暴露量的2.6至7.2倍,导致流产,死产,早产的剂量相关增加(相应降低出生体重) ,并增加婴儿死亡率。此外,在子宫内暴露的两只幼猴的泌尿生殖系统中发现发育异常至30 mg / kg的ipilimumab(在3 mg / kg的剂量下,人类AUC的7.2倍)。一只雌性婴儿猴子的左肾和输尿管有单侧肾发育不全,而一只雄性婴儿猴子的尿道无孔,伴有尿路阻塞和皮下阴囊水肿。
遗传工程小鼠杂CTLA-4(CTLA-4 +/-),目标为易普利姆玛,出现健康和生下健康CTLA-4 +/-杂合子的后代。交配的CTLA-4 +/-杂合小鼠也产生了缺乏CTLA-4的后代(纯合子阴性,CTLA-4-/-)。CTLA-4-/-纯合子阴性婴儿出生时健康,在2周龄时表现出多器官淋巴增生性疾病的征兆,在3至4周龄时全部死亡,并伴有大量淋巴细胞增殖和多器官组织破坏。
8.2哺乳
风险摘要
尚不清楚母乳中是否存在耶尔沃伊。在猴子中,牛奶中存在ipilimumab (请参见数据)。没有数据可以评估耶尔沃伊对牛奶产量的影响。劝告妇女在接受YERVOY治疗期间以及最终剂量后3个月内停止母乳喂养。
数据
在以3 mg / kg剂量暴露于人的剂量水平下处理过的猴子中,ipilimumab在牛奶中的浓度分别为0.1 mcg / mL和0.4 mcg / mL,其比例最高可达人类的2.6和7.2倍。药物稳态血清浓度的0.3%。
8.3生殖潜力的男性和女性
避孕
基于其作用机理,当施予孕妇时,YERVOY可能引起胎儿伤害[见在特定人群中使用(8.1) ]。建议有生殖潜力的女性在接受YERVOY治疗期间以及最后一次服用YERVOY后3个月内使用有效的避孕方法。
8.4小儿使用
YERVOY已在12岁及12岁以上的小儿患者中确立了其安全性和有效性,可用于治疗无法切除或转移的黑色素瘤或治疗微卫星不稳定性高(MSI-H)或错配修复缺陷(dMMR)转移性结直肠癌氟嘧啶,奥沙利铂和伊立替康治疗后进展。成年人对YERVOY的充分和良好对照的研究以及人群药代动力学数据的证据支持了YERVOY在该年龄段的使用,表明在儿科和成人人群中3 mg / kg和1 mg / kg的剂量可比较。此外,
对于12岁及12岁以上的小儿患者,尚无用于辅助治疗黑色素瘤或治疗肾细胞癌的安全性和有效性。此外,对于任何小于12岁的小儿患者,YERVOY尚未确定其安全性和有效性。
在两项临床试验中,总共对45名儿科患者进行了YERVOY评估。在一项剂量寻找试验中,对33例复发或难治性实体瘤的儿科患者进行了评估。中位年龄为13岁(范围为2到21岁),并且20例≥12岁。每3周以90、3分钟,1、3、5和10 mg / kg的剂量静脉注射YERVOY,共4剂,然后每12周一次,直至进展或治疗中止。
在一项开放性单臂试验中,还对12例≥12岁(范围为12至16岁)的先前治疗或未经治疗的,不可切除的3或4期恶性黑色素瘤患儿进行了YERVOY评估。患者每3周90分钟静脉注射3毫克/千克(4例患者)或10毫克/千克(8例患者)的YERVOY,共4剂。
在两项研究中,在接受YERVOY治疗的17例年龄≥12岁的黑色素瘤患者中,两名患者经历了客观反应,包括持续16个月的部分反应。非黑色素瘤实体瘤患者无反应。
YERVOY在儿童和青少年中的总体安全性与成人的安全性一致。
小儿药代动力学(PK)
基于人口PK分析,该研究使用了来自4个2期2期成人研究(N = 521)和2个儿科研究(N = 44)的565位患者的可用汇总数据,在成人和儿科患者中,依匹木单抗的体重标准化清除率相当。在每3周一次给药方案为3 mg / kg的儿科患者中,模型模拟的ipilimumab稳态血药浓度和谷值几何平均值(CV%)为65.8(17.6%)和20.7(33.1%)mcg / mL (适用于2至6岁的儿童),70.1(19.6%)和19.6(42.9%)mcg / mL(适用于6至<12岁的儿童),73.3(20.6%)和17.8(50.8%)mcg / mL(适用于12岁及12岁以上),与成人患者的水平相当。
8.5老年人使用
在MDX010-20中的511例接受YERVOY治疗的患者(不可切除或转移性黑色素瘤)中,有28%年龄在65岁及以上。在老年患者(65岁及以上)和年轻患者(小于65岁)之间,没有安全性或疗效的总体差异。
CA184-029(黑色素瘤的辅助治疗)和CHECKMATE-142(转移性结直肠癌)未包括足够多的65岁及65岁以上的患者来确定他们是否与年轻患者有所不同。
在CHECKMATE-214(肾细胞癌)中随机分配给nivolumab 3 mg / kg并给予YERVOY 1 mg / kg的550名患者中,38%为65岁或以上,8%为75岁或以上。在老年患者和年轻患者之间,没有安全性的总体差异报告。在中度或低风险的老年患者中,没有报道疗效的总体差异。
8.6肾功能不全
肾功能不全患者无需调整剂量[见临床药理学(12.3) ]。
8.7肝功能不全
轻度肝功能不全(总胆红素[TB]>正常上限[ULN]上限的1.0至1.5倍或AST> ULN上限)的患者无需调整剂量。尚未对中度(TB> 1.5至3.0倍ULN和任何AST)或严重(TB> 3倍ULN和任何AST)肝功能不全的患者进行YERVOY的研究[见临床药理学(12.3) ]。
10过量
没有关于YERVOY用药过量的信息。
11说明
伊匹木单抗是一种重组人单克隆抗体,可与细胞毒性T淋巴细胞相关抗原4(CTLA-4)结合。伊匹木单抗是一种IgG1 kappa免疫球蛋白,分子量约为148 kDa。伊匹木单抗是在哺乳动物(中国仓鼠卵巢)细胞培养物中产生的。
YERVOY是一种无菌,无防腐剂,澄清至微乳白色,无色至浅黄色的静脉输液,其中可能含有少量可见的半透明至白色无定形伊立木单抗颗粒。它以50 mg / 10 mL和200 mg / 40 mL的一次性小瓶形式提供。每毫升含有5毫克的ipilimumab和以下非活性成分:二亚乙基三胺五乙酸(DTPA)(0.04毫克),甘露醇(10毫克),聚山梨酯80(植物性)(0.1毫克),氯化钠(5.85毫克),三盐酸(3.15 mg)和注射用水(USP),pH值为7。
12临床药理学
12.1行动机制
CTLA-4是T细胞活性的负调节剂。伊匹木单抗是一种单克隆抗体,可与CTLA-4结合并阻断CTLA-4及其配体CD80 / CD86的相互作用。已显示对CTLA-4的阻断可增强T细胞的活化和增殖,包括肿瘤浸润性T效应细胞的活化和增殖。抑制CTLA-4信号传导也可以降低T调节细胞功能,这可能有助于T细胞反应性(包括抗肿瘤免疫反应)的普遍增加。
12.3药代动力学
在785例不可切除或转移性黑色素瘤患者中,对ipilimumab的药代动力学(PK)进行了研究,每3周一次接受4剂0.3、3或10 mg / kg的剂量。伊匹木单抗的PK 在0.3至10 mg / kg的剂量范围内是线性的。每3周施用一次YERVOY后,全身蓄积为1.5倍以下。第三剂达到伊立木单抗的稳态浓度;稳定状态下的平均C min每3周为3 mg / kg时为19.4 mcg / mL,10 mg / kg时为58.1 mcg / mL。基于种群PK分析的终末半衰期(t 1/2)的平均值(t 1/2)为15.4天(34%),清除率(CL)为16.8 mL / h(38%)。
YERVOY含纳武单抗:与单独给药YERVOY相比,当将YERVOY 1 mg / kg与nivolumab 3 mg / kg联合给药时,依匹莫单抗和nivolumab 的CL 不变。
当联合给药时,的CL 易普利姆玛是抗的存在不变易普利姆玛的抗体和nivolumab的CL在抗nivolumab抗体的存在增加了20%。
特定人群
在人群PK分析中评估了各种协变量对ipilimumab PK的影响。依匹莫单抗的CL 随体重增加而增加,从而支持基于推荐体重(mg / kg)的给药。以下因素对依匹莫单抗的CL无临床重要影响:年龄(范围:23至88岁),性别,工作状态,肾功能不全,轻度肝功能不全,既往的癌症治疗方法和基线乳酸脱氢酶(LDH)水平。由于非高加索族的可用数据有限,因此未检查种族的影响。
肾功能不全:在轻度(GFR <90和≥60mL / min / 1.73 m 2; n = 349),中度(GFR <60和≥30mL / min)的患者中评估了肾功能不全对ipilimumab CL的影响与肾功能正常(GFR≥90mL / min / 1.73 m的患者)相比,/ 1.73 m 2; n = 82)或严重(GFR <30且≥15mL / min / 1.73 m 2; n = 4)肾功能不全2; n = 350)的人口PK分析。在肾功能不全的患者和肾功能正常的患者之间,没有发现伊匹木单抗 CL的临床上重要的临床差异[见特定人群的使用(8.6) ]。
肝功能不全:在人群PK分析中,与肝功能正常(n = 708)的患者相比,轻度肝功能不全(n = 708)的患者评估了肝功能不全对ipilimumab CL的影响,且在临床上无重要临床差异。发现伊立木单抗的CL 。尚未对中度或重度肝功能不全患者进行YERVOY的研究[请参见在特定人群中使用(8.7) ]。
小儿人口:[见在特定人群中使用(8.4) ]。
13毒理学
13.1致癌,诱变,生育力受损
长期动物研究尚未评估ipilimumab的致癌潜力,也未评估ipilimumab的遗传毒性。
依匹莫单抗尚未进行生育力研究。
14临床研究
14.1不可切除或转移性黑色素瘤
在一项随机(3:1:1),双盲,双模拟试验(MDX010-20,NCT00094653)中对YERVOY的安全性和有效性进行了研究,该试验包括676名先前接受过一种或多种治疗的不可切除或转移性黑素瘤患者。下列物质之一:醛固酮,达卡巴嗪,替莫唑胺,福美汀或卡铂。在这676名患者中,有403名患者随机接受了不完全弗氏佐剂(gp100)的研究性肽疫苗联合接受3 mg / kg的YERVOY,137名患者被随机接受了3 mg / kg接受YERVOY的研究,而136名患者被随机接受了gp100作为单一代理。该试验仅招募了具有HLA-A2 * 0201基因型的患者。这种HLA基因型有助于研究性肽疫苗的免疫提呈。该试验排除了患有活动性自身免疫疾病或接受全身免疫抑制的器官移植患者。每3周以3 mg / kg的剂量静脉注射YERVOY /安慰剂,共4剂。每3周一次深度皮下注射,以2 mg肽的剂量给予Gp100 /安慰剂,共4剂。在第12和24周以及此后每3个月进行肿瘤反应的评估。在第12或24周有客观肿瘤反应证据的患者,分别评估其在16或28周时的持久性确认。在第12和24周以及此后每3个月进行肿瘤反应的评估。在第12或24周有客观肿瘤反应证据的患者,分别评估其在16或28周时的持久性确认。在第12和24周以及此后每3个月进行肿瘤反应的评估。在第12或24周有客观肿瘤反应证据的患者,分别评估其在16或28周时的持久性确认。
主要功效结局指标是YERVOY plus gp100组的总生存期(OS)与单药gp100组的总生存期(OS)。次要疗效结局指标包括:YERVOY plus gp100组的OS与YERVOY组的OS,YERVOY组的OS与gp100组的OS,每个试验组之间第24周的最佳总体缓解率(BORR) 。
在随机分组的患者中,YERVOY加gp100,YERVOY和gp100组的男性分别为61%,59%和54%。29%的年龄≥65岁,中位年龄为57岁,71%患有M1c分期,12%曾接受过脑转移治疗,98%的ECOG表现为0和1,23%接受过aldesleukin和38%的LDH水平升高。随机分配到任一装有YERVOY的手臂的患者中有61%接受了所有4种计划剂量。中位随访时间为8.9个月。
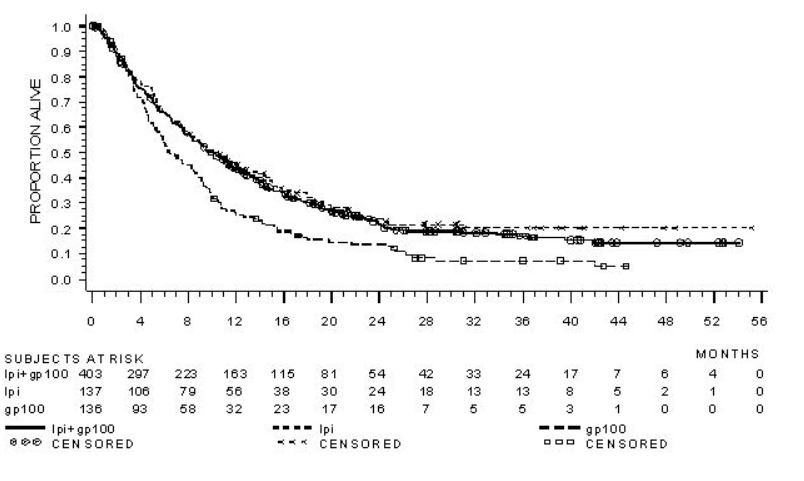
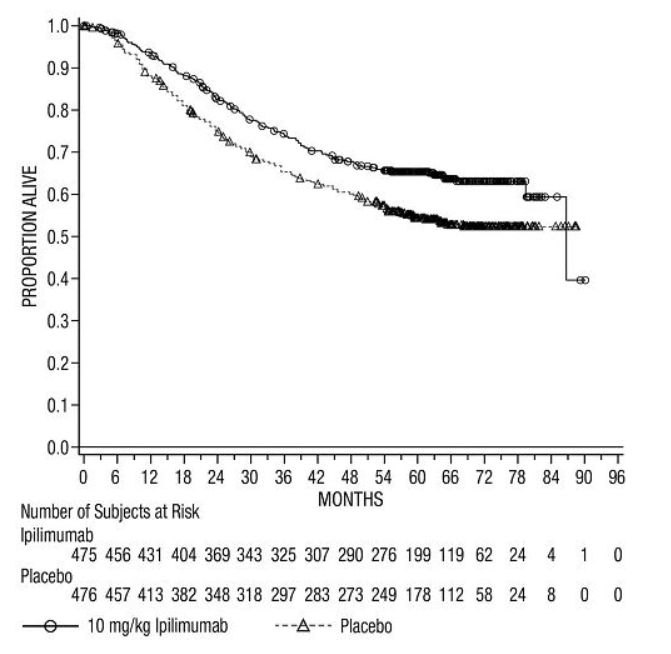
操作系统结果如表11和图1所示。
表11:总体生存结果
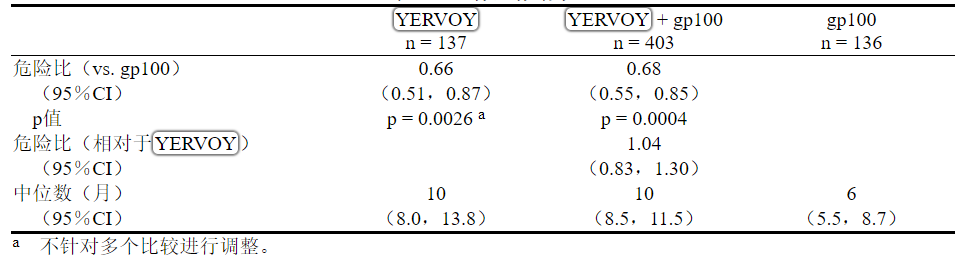
图1:总体生存
研究人员评估的最佳总体反应率(BORR)在YERVOY plus gp100组中为5.7%(95%CI:3.7%,8.4%),在YERVOY中为10.9%(95%CI:6.3%,17.4%)臂和gp100臂中的1.5%(95%CI:0.2%,5.2%)。YERVOY加gp100组的中位反应持续时间为11.5个月,而YERVOY或gp100组的中位反应持续时间尚未达到。
14.2黑色素瘤的辅助治疗
在CA184-029(NCT00636168)中对YERVOY在黑色素瘤辅助治疗中的安全性和有效性进行了研究,这是一项随机(1:1),双盲,安慰剂对照试验,用于切除IIIA期(结节累及1mm以上)的患者),IIIB和IIIC(无转运中)在组织学上证实为皮肤黑色素瘤。患者每3周随机接受YERVOY 10 mg / kg或安慰剂静脉输注,共4剂,然后从第24周至156周(3年)每12周一次接受YERVOY 10 mg / kg或安慰剂,直到记录到疾病复发或不可接受的毒性。入选前需要在随机分组前12周内用全淋巴结清扫术彻底切除黑色素瘤。既往曾接受过黑色素瘤,自身免疫性疾病的治疗,且先前或同时使用过免疫抑制剂的患者不符合资格。根据美国癌症联合委员会(AJCC)2002分类按阶段进行随机分层(IIIA期结节累及> 1 mm,IIIB期,IIIC期累及1至3个淋巴结,IIIC期≥4个淋巴结)和按地区(北美,欧洲和澳大利亚)。主要疗效结局指标是独立审查委员会(IRC)评估的无复发生存期(RFS),定义为随机化日期与首次复发最早的时间(局部,区域或远处转移)或死亡之间的时间,和整体生存。在最初的3年中,每12周进行一次肿瘤评估,然后每24周进行一次肿瘤评估,直到远处复发为止。1 mm淋巴结受累,IIIB期,IIIC期有1至3个淋巴结受累,IIIC期≥4个受累淋巴结)和按地区(北美,欧洲和澳大利亚)。主要疗效结局指标是独立审查委员会(IRC)评估的无复发生存期(RFS),定义为随机化日期与首次复发最早的时间(局部,区域或远处转移)或死亡之间的时间,和整体生存。在最初的3年中,每12周进行一次肿瘤评估,然后每24周进行一次肿瘤评估,直到远处复发为止。1 mm淋巴结受累,IIIB期,IIIC期有1至3个淋巴结受累,IIIC期≥4个受累淋巴结)和按地区(北美,欧洲和澳大利亚)。主要疗效结局指标是独立审查委员会(IRC)评估的无复发生存期(RFS),定义为随机化日期与首次复发最早的时间(局部,区域或远处转移)或死亡之间的时间,和整体生存。在最初的3年中,每12周进行一次肿瘤评估,然后每24周进行一次肿瘤评估,直到远处复发为止。定义为随机化日期与首次复发最早的日期(局部,区域或远处转移)或死亡之间的时间,以及总体生存期。在最初的3年中,每12周进行一次肿瘤评估,然后每24周进行一次肿瘤评估,直到远处复发为止。定义为随机化日期与首次复发最早的日期(局部,区域或远处转移)或死亡之间的时间,以及总体生存期。在最初的3年中,每12周进行一次肿瘤评估,然后每24周进行一次肿瘤评估,直到远处复发为止。
在951名患者中,有475名被随机分配接受YERVOY治疗,而476名则接受了安慰剂治疗。中位年龄为51岁(范围:18至84岁),男性62%,白人99%,ECOG表现为0的为94%。就疾病分期而言,有20%的IIIA期淋巴结> 1毫米,44%的患者处于IIIB期,而36%的患者处于IIIC期(无在途转移)。该试验人群的其他疾病特征是:临床上可触及的淋巴结(58%),2个或更多阳性淋巴结(54%)和溃疡性原发灶(42%)。
功效结果在表12和图2中。
表12:CA184-029中的功效结果
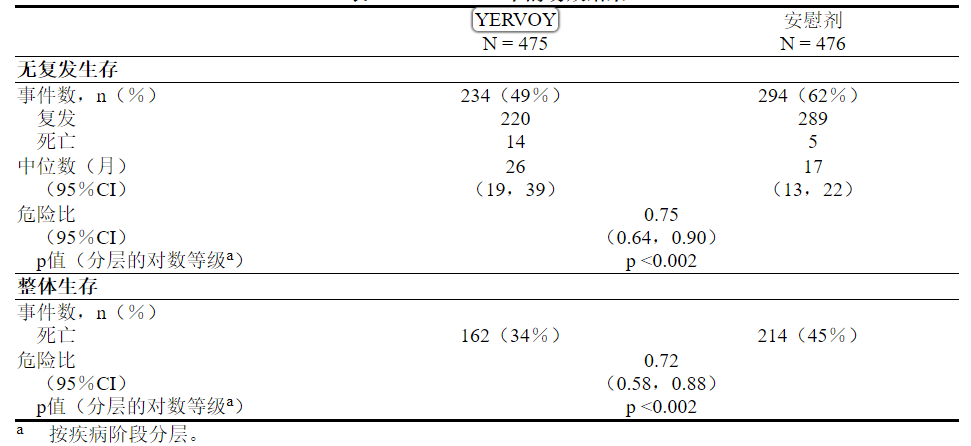
图2:总体生存
14.3先前未经治疗的晚期肾细胞癌
CHECKMATE-214(NCT02231749)是一项针对先前未接受治疗的晚期RCC患者的随机(1:1)开放标签研究。不论患者的PD-L1状态如何,都将其包括在内。CHECKMATE-214排除了具有任何历史或同时发生脑转移,活动性自身免疫疾病或需要全身免疫抑制的医疗状况的患者。根据国际转移RCC数据库联合会(IMDC)的预后评分和区域对患者进行分层。
根据IMDC标准(至少从最初的肾细胞癌诊断至随机分组,卡诺夫斯基机能状态<80%,血红蛋白不足一年),对具有6种预后危险因素中的至少一种或多种的中度/低危患者进行疗效评估小于正常下限,校正钙大于10 mg / dL,血小板计数大于正常上限,绝对中性粒细胞计数大于正常上限)。
患者被随机分配至每3周静脉给予3毫克尼伏鲁单抗加3mg / kg的YERVOY(n = 425),共4剂,然后每两周随机给予nivolumab单药3 mg / kg或口服舒尼替尼(n = 422)50每天一次,每次4毫克,然后每星期休息2星期。继续治疗直至疾病进展或不可接受的毒性。
中位年龄为61岁(范围:21至85),其中38%≥65岁和8%≥75岁。大多数患者为男性(73%)和白人(87%),分别有26%和74%的患者的基线KPS分别为70%至80%和90%至100%。
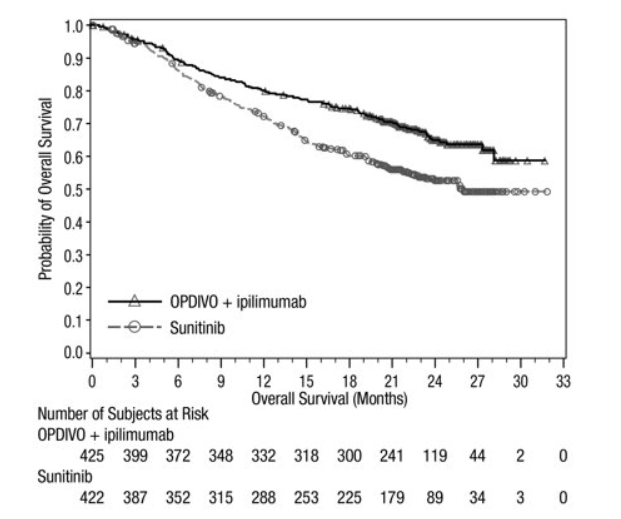
在中/低危患者中,主要疗效指标为OS,PFS(IRRC评估)和确诊ORR(IRRC评估)。在该人群中,该试验证明,与舒尼替尼相比,随机分配给尼古拉单抗+ YERVOY的患者的OS和ORR有统计学意义的改善(表13和图3)。无论PD-L1表达水平如何,都可观察到OS获益。该试验未证明PFS有统计学上的显着改善。
表13和图3列出了CHECKMATE-214的功效结果。
表13:疗效结果-CHECKMATE-214
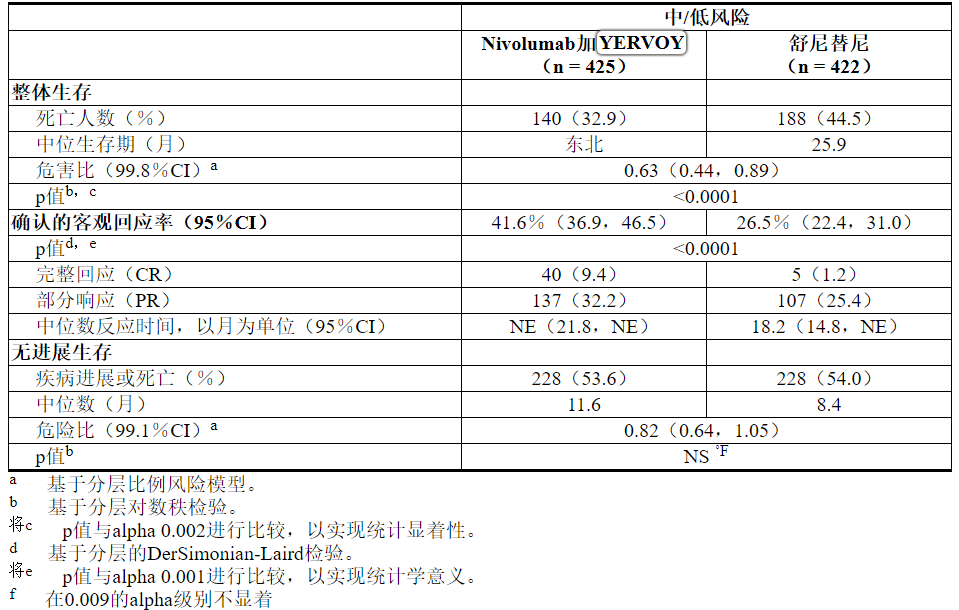
图3:总生存期(中/低风险人群)-CHECKMATE-214
根据IMDC标准,CHECKMATE-214还将249名有风险的患者随机分为nivolumab加YERVOY(n = 125)或舒尼替尼(n = 124)。这些患者未作为疗效分析人群的一部分进行评估。与舒尼替尼相比,接受nivolumab加YERVOY的风险较高的患者的OS风险比为1.45(95%CI:0.75,2.81)。尚未确定nivolumab加YERVOY在先前未治疗的具有良好风险疾病的肾细胞癌中的疗效。
14.4高微卫星不稳定性(MSI-H)或错配修复缺陷(dMMR)转移性结直肠癌
CHECKMATE-142(NCT02060188)是一项多中心,非随机,多队列并行,开放标签研究,研究对象为在局部接受dMMR或MSI-H转移性CRC(mCRC)的患者中,在接受氟嘧啶治疗之前或之后疾病发展-,奥沙利铂或伊立替康为主的化疗。关键的资格标准是至少一种转移性疾病,ECOG PS 0或1的既往治疗方法,并且不存在以下各项:活动性脑转移,活动性自身免疫性疾病或需要全身免疫抑制的医疗状况。
参加YERVOY和nivolumab MSI-H mCRC队列的患者每3周接受4剂剂量的YERVOY 1 mg / kg和nivolumab 3 mg / kg静脉内注射,然后每2周接受一次ivolumab 3 mg / kg IV作为单一药物。参加单药nivolumab MSI-H mCRC队列的患者每2周通过静脉(IV)输注接受3 mg / kg的nivolumab。两组患者均继续治疗,直至出现不可接受的毒性或影像学进展。
在最初的24周中每6周进行一次肿瘤评估,此后每12周进行一次肿瘤评估。疗效结局指标为独立放射线照相审查委员会(IRRC)使用实体瘤反应评估标准(RECIST v1.1)和反应持续时间(DOR)评估的总体反应率(ORR)。
共有119名患者参加了YERVOY联合nivolumab队列研究。中位年龄为58岁(范围:21至88岁),其中32%≥65岁和9%≥75岁;男性为59%,白人为92%。基线ECOG PS为0(45%)或1(55%),据报道有29%患有Lynch综合征。在整个队列中,有69%的人接受过氟嘧啶,奥沙利铂和伊立替康的治疗;分别有10%,40%,24%和15%的患者接受过1、2、3或≥4种转移性疾病的先前治疗,而29%的患者接受了抗EGFR抗体。
共有74位患者参加了单药nivolumab队列研究。中位年龄为53岁(范围:26至79岁),其中23%≥65岁且5%≥75岁,男性59%,白人88%。基线ECOG表现状态为0(43%),1(55%)或3(1.4%),据报道有Lynch综合征为36%。在74例患者中,有72%接受过氟嘧啶,奥沙利铂和伊立替康治疗。分别有7%,30%,28%,19%和16%的患者接受过0、1、2、3或≥4种转移性疾病的既往治疗,其中42%的患者接受了抗EGFR抗体。
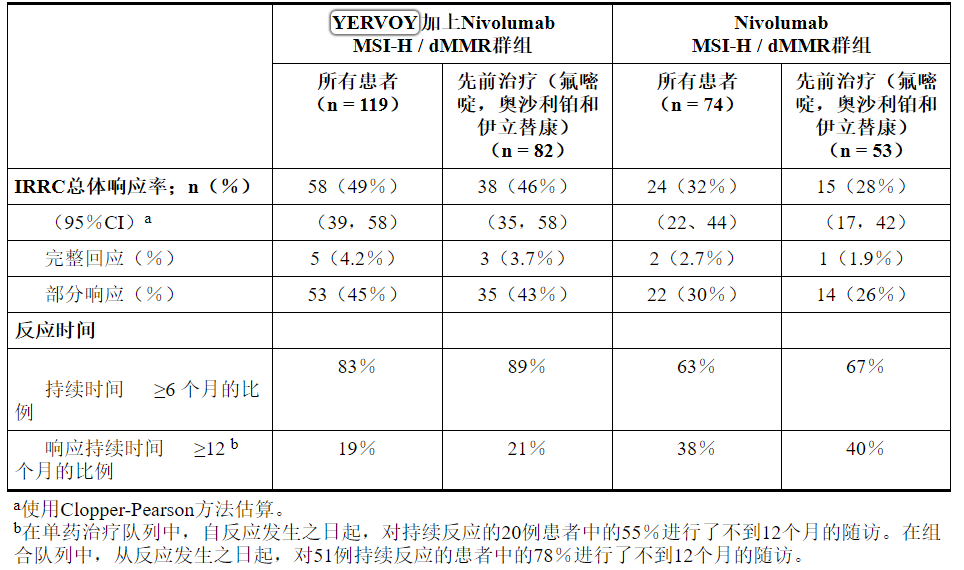
疗效结果见表14。
表14:CHECKMATE-142中的功效结果
16供应/存储和处理方式
YERVOY(易普利姆玛)注射剂可如下:
将YERVOY储存在2°C至8°C(36°F至46°F)的冷藏条件下。将YERVOY存放在原始纸箱中直至使用,以防光照。请勿冻结或摇动。
17患者咨询信息
建议患者阅读FDA批准的患者标签(用药指南)。
免疫介导的不良反应
告知患者可能需要皮质类固醇治疗以及停用或停用YERVOY的免疫介导的不良反应的风险,包括:
• 肠结肠炎/结肠炎:建议患者因腹泻或严重腹痛立即联系其医疗保健提供者[请参阅警告和注意事项(5.1) ]。
• 肝炎:建议患者立即就黄疸,严重的恶心或呕吐,腹部右侧疼痛,嗜睡或容易瘀伤或流血与医生联系[请参阅警告和注意事项(5.2) ]。
• 皮肤不良反应:建议患者立即联系其医护人员以预防皮疹[见警告和注意事项(5.3) ]。
• 神经病:建议患者立即联系其医疗保健提供者以应对神经病[见警告和注意事项(5.4) ]。
• 内分泌疾病:建议患者就垂体炎,肾上腺皮质功能不全,甲状腺功能减退,甲状腺功能亢进和糖尿病的体征或症状立即联系其医疗保健提供者[请参阅警告和注意事项(5.5) ]。
• 肺炎:建议患者如果出现任何新的或恶化的咳嗽,胸痛或呼吸急促,请立即与他们的医疗保健提供者联系[请参阅警告和注意事项(5.6) ]。
• 肾炎和肾功能不全:建议患者就肾炎的体征或症状立即与医护人员联系,包括尿量减少,尿中血液,脚踝肿胀,食欲不振以及肾功能不全的任何其他症状[请参阅警告和注意事项(5.7 ) ]。
• 脑炎:建议患者立即就其脑炎的神经系统症状或体征与他们的医疗保健提供者联系[请参阅警告和注意事项(5.8) ]。
输液反应
• 告知患者潜在的输注反应风险[请参阅警告和注意事项(5.9) ]。
女性生殖潜能
• 告知女性患者,YERVOY可能导致胎儿伤害。劝告有生殖潜力的女性在接受YERVOY治疗期间以及最后一次给药后的3个月内使用有效的避孕方法(请参见“ 在特定人群中使用(8.3) ”)。
• 建议女性患者在已知或怀疑怀孕的情况下联系其医疗保健提供者。谁可能怀孕到接触施贵宝期间1-800-721-5072暴露于YERVOY指教雌性[见警告和注意事项(5.11)和特殊人群中使用(8.1,8.3) ]。告知患者,有一项孕期安全性监视研究可以监测怀孕期间暴露于YERVOY的妇女的妊娠结局,可以致电1-844-593-7869来招募他们[请参阅在特定人群中使用(8.1) ]。
哺乳期
• 劝告妇女在使用耶尔伏伊治疗期间以及最后一次给药后的三个月内不要母乳喂养[见在特定人群中使用(8.2) ]。
制造商:
百时美施贵宝公司
普林斯顿,新泽西州08543美国
美国牌照号1713[打印代码]

本药物指南已获得美国食品和药物管理局的批准。
修订日期:2019年5月YERVOY 50 mg / 10 mL代表性包装
有关YERVOY可用软件包的完整列表,请参见“ 如何提供”部分。
NDC 0003-2327-11
仅Rx
YERVOY ®
(易普利姆玛)
注射
50毫克/毫升10
(5毫克/毫升)
用于静脉内输注仅
单次使用的小瓶; 丢弃
每位患者的分配封闭式用药指南
百时美施贵宝
YERVOY 200 mg / 40 mL代表性包装
NDC 0003-2328-22
仅Rx
YERVOY ®
(易普利姆玛)
注射
200毫克/毫升40
(5毫克/毫升)
用于静脉内输注仅
单次使用的小瓶; 丢弃
每位患者的分配封闭式用药指南
百时美施贵宝
【备注】以上内容仅供参考,不作为用药依据,详情请参照药品附带说明书。
-
本说明书来源于:美国FDA
https://nctr-crs.fda.gov/fdalabel/services/spl/set-ids/2265ef30-253e-11df-8a39-0800200c9a66/spl-doc?hl=YERVOY
温馨提醒:
①建议您用 谷歌浏览器 在电脑上或手机 打开以上链接,就可以自动翻译成简体中文,而且翻译的还比较准确。
②本说明书仅供参考,最新的说明书详见药品附带的说明书。
WARNING: IMMUNE-MEDIATED ADVERSE REACTIONS
YERVOY can result in severe and fatal immune-mediated adverse reactions. These immune-mediated reactions may involve any organ system; however, the most common severe immune-mediated adverse reactions are enterocolitis, hepatitis, dermatitis (including toxic epidermal necrolysis), neuropathy, and endocrinopathy. The majority of these immune-mediated reactions initially manifested during treatment; however, a minority occurred weeks to months after discontinuation of YERVOY.
Permanently discontinue YERVOY and initiate systemic high-dose corticosteroid therapy for severe immune-mediated reactions [see Dosage and Administration (2.5)].
Assess patients for signs and symptoms of enterocolitis, dermatitis, neuropathy, and endocrinopathy, and evaluate clinical chemistries including liver function tests, adrenocorticotropic hormone (ACTH) level, and thyroid function tests, at baseline and before each dose [see Warnings and Precautions (5.1, 5.2, 5.3, 5.4, 5.5)].
1 INDICATIONS AND USAGE
1.1 Unresectable or Metastatic Melanoma
YERVOY is indicated for the treatment of unresectable or metastatic melanoma in adults and pediatric patients (12 years and older) [see Clinical Studies (14.1)].
1.2 Adjuvant Treatment of Melanoma
YERVOY is indicated for the adjuvant treatment of patients with cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm who have undergone complete resection, including total lymphadenectomy [see Clinical Studies (14.2)].
1.3 Advanced Renal Cell Carcinoma
YERVOY, in combination with nivolumab, is indicated for the treatment of patients with intermediate or poor-risk, previously untreated advanced renal cell carcinoma (RCC) [see Clinical Studies (14.3)].
1.4 Microsatellite Instability-High (MSI-H) or Mismatch Repair Deficient (dMMR) Metastatic Colorectal Cancer
YERVOY, in combination with nivolumab, is indicated for the treatment of adult and pediatric patients 12 years of age and older with microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer (CRC) that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan [see Clinical Studies (14.4)]. This indication is approved under accelerated approval based on overall response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosing for Unresectable or Metastatic Melanoma
The recommended dose of YERVOY is 3 mg/kg administered intravenously (IV) over 90 minutes every 3 weeks for a maximum of 4 doses. In the event of toxicity, doses may be delayed, but all treatment must be administered within 16 weeks of the first dose [see Clinical Studies (14.1)].
2.2 Recommended Dosing for Adjuvant Treatment of Melanoma
The recommended dose of YERVOY is 10 mg/kg administered IV over 90 minutes every 3 weeks for 4 doses followed by 10 mg/kg every 12 weeks for up to 3 years [see Clinical Studies (14.2)]. In the event of toxicity, doses are omitted, not delayed.
2.3 Recommended Dosing for RCC
The recommended dose of YERVOY in combination with nivolumab is nivolumab 3 mg/kg administered as an intravenous infusion over 30 minutes, followed by YERVOY 1 mg/kg administered as an intravenous infusion over 30 minutes on the same day, every 3 weeks for 4 doses [see Clinical Studies (14.3)]. After completing 4 doses of the combination, administer nivolumab as a single agent, either:
• 240 mg every 2 weeks, or
• 480 mg every 4 weeks
as an intravenous infusion over 30 minutes until disease progression or unacceptable toxicity. Review the Prescribing Information for nivolumab prior to initiation.
2.4 Recommended Dosing for Colorectal Cancer
The recommended dose of YERVOY is:
• YERVOY 1 mg/kg administered as an intravenous infusion over 30 minutes, immediately following nivolumab administered on the same day, every 3 weeks for up to 4 doses or until intolerable toxicity or disease progression [see Clinical Studies (14.4)]. Review the Prescribing Information for nivolumab prior to initiation.
2.5 Recommended Dose Modifications
Recommendations for YERVOY modifications are provided in Table 1. When YERVOY is administered in combination with nivolumab, if YERVOY is withheld, nivolumab should also be withheld. Review the Prescribing Information for nivolumab for recommended dose modifications.
Interrupt or slow the rate of infusion in patients with mild or moderate infusion reactions. Discontinue in patients with severe or life-threatening infusion reactions.
Table 1: Recommended Treatment Modifications for Immune-Mediated Adverse Reactions of YERVOY
2.6 Preparation and Administration
• Do not shake product.
• Inspect parenteral drug products visually for particulate matter and discoloration prior to administration. Discard vial if solution is cloudy, there is pronounced discoloration (solution may have pale-yellow color), or there is foreign particulate matter other than translucent-to-white, amorphous particles.
Preparation of Solution
• Allow the vials to stand at room temperature for approximately 5 minutes prior to preparation of infusion.
• Withdraw the required volume of YERVOY and transfer into an intravenous bag.
• Dilute with 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to prepare a diluted solution with a final concentration ranging from 1 mg/mL to 2 mg/mL. Mix diluted solution by gentle inversion.
• Store the diluted solution for no more than 24 hours under refrigeration (2°C to 8°C, 36°F to 46°F) or at room temperature (20°C to 25°C, 68°F to 77°F).
• Discard partially used vials or empty vials of YERVOY.
Administration Instructions
• Do not mix YERVOY with, or administer as an infusion with, other medicinal products.
• Flush the intravenous line with 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP after each dose.
• Administer diluted solution over 90 minutes through an intravenous line containing a sterile, non-pyrogenic, low-protein-binding in-line filter.
When administered in combination with nivolumab, infuse nivolumab first followed by YERVOY on the same day. Use separate infusion bags and filters for each infusion.
3 DOSAGE FORMS AND STRENGTHS
Injection: 50 mg/10 mL (5 mg/mL) and 200 mg/40 mL (5 mg/mL) as a clear to slightly opalescent, colorless to pale-yellow solution in a single-use vial.
4 CONTRAINDICATIONS
None.
5 WARNINGS AND PRECAUTIONS
YERVOY can result in severe and fatal immune-mediated reactions [see Boxed Warning].
5.1 Immune-Mediated Enterocolitis/Colitis
Immune-mediated enterocolitis, including fatal cases, can occur with YERVOY.
Monitor patients for signs and symptoms of enterocolitis (such as diarrhea, abdominal pain, mucus or blood in stool, with or without fever) and of bowel perforation (such as peritoneal signs and ileus). In symptomatic patients, rule out infectious etiologies and consider endoscopic evaluation for persistent or severe symptoms. Cytomegalovirus (CMV) infection/reactivation has been reported in patients with corticosteroid-refractory immune-mediated colitis. In cases of corticosteroid-refractory colitis, consider repeating an infectious workup to exclude alternative etiologies. Addition of an alternative immunosuppressive agent to the corticosteroid therapy, or replacement of the corticosteroid therapy should be considered in corticosteroid-refractory immune-mediated colitis if other causes are excluded.
Permanently discontinue YERVOY in patients with severe enterocolitis and initiate systemic corticosteroids at a dose of 1 to 2 mg/kg/day of prednisone or equivalent. Upon improvement to Grade 1 or less, initiate corticosteroid taper and continue to taper over at least 1 month. In clinical trials, rapid corticosteroid tapering resulted in recurrence or worsening symptoms of enterocolitis in some patients. Consider adding anti-TNF or other immunosuppressant agents for management of immune-mediated enterocolitis unresponsive to systemic corticosteroids within 3 to 5 days or recurring after symptom improvement, if other causes are excluded.
Withhold YERVOY dosing for moderate enterocolitis; administer anti-diarrheal treatment and, if persistent for more than 1 week, initiate systemic corticosteroids at a dose of 0.5 mg/kg/day prednisone or equivalent [see Dosage and Administration (2.5)].
YERVOY as a Single Agent
Metastatic Melanoma
In patients receiving YERVOY 3 mg/kg in MDX010-20 (NCT00094653), severe, life-threatening, or fatal (diarrhea of 7 or more stools above baseline, fever, ileus, peritoneal signs; Grade 3 to 5) immune-mediated enterocolitis occurred in 34 YERVOY-treated patients (7%), and moderate (diarrhea with up to 6 stools above baseline, abdominal pain, mucus or blood in stool; Grade 2) enterocolitis occurred in 28 YERVOY-treated patients (5%). Across all YERVOY-treated patients (n=511), 5 patients (1%) developed intestinal perforation, 4 patients (0.8%) died as a result of complications, and 26 patients (5%) were hospitalized for severe enterocolitis.
The median time to onset of Grade 3 to 5 enterocolitis was 1.7 months (range: 11 days to 3.1 months) and for Grade 2 enterocolitis was 1.4 months (range: 2 days to 4.3 months).
Twenty-nine patients (85%) with Grade 3 to 5 enterocolitis were treated with high-dose (≥40 mg prednisone equivalent per day) corticosteroids, with a median dose of 80 mg/day of prednisone or equivalent; the median duration of treatment was 16 days (ranging up to 3.2 months) followed by corticosteroid taper. Of the 28 patients with moderate enterocolitis, 46% were not treated with systemic corticosteroids, 29% were treated with <40 mg prednisone or equivalent per day for a median duration of 1.2 months, and 25% were treated with high-dose corticosteroids for a median duration of 10 days prior to corticosteroid taper. Infliximab was administered to 5 (8%) of the 62 patients with moderate, severe, or life-threatening immune-mediated enterocolitis following inadequate response to corticosteroids.
Of the 34 patients with Grade 3 to 5 enterocolitis, 74% experienced complete resolution, 3% experienced improvement to Grade 2 severity, and 24% did not improve. Among the 28 patients with Grade 2 enterocolitis, 79% experienced complete resolution, 11% improved, and 11% did not improve.
Adjuvant Treatment of Melanoma
In patients receiving YERVOY 10 mg/kg in CA184-029 (NCT00636168), Grade 3 to 5 immune-mediated enterocolitis occurred in 76 patients (16%) and Grade 2 enterocolitis occurred in 68 patients (14%). Seven patients (1.5%) developed intestinal perforation and 3 patients (0.6%) died as a result of complications [see Adverse Reactions (6.1)].
The median time to onset for Grade 3 to 4 enterocolitis was 1.1 months (range: 1 day to 33.1 months) and for Grade 2 enterocolitis was 1.1 months (range: 1 day to 20.6 months).
Seventy-one patients (95%) with Grade 3 to 4 enterocolitis were treated with systemic corticosteroids. The median duration of treatment was 4.7 months (ranging up to 52.3 months).
Of the 68 patients with moderate enterocolitis, 51 patients (75%) were treated with systemic corticosteroids with a median duration of treatment of 3.5 months (ranging up to 52.2 months). Non-corticosteroids immunosuppression, consisting almost exclusively of infliximab, was used to treat 36% of patients with Grade 3 to 4 enterocolitis and 15% of patients with a Grade 2 event.
Of the 75 patients with Grade 3 to 4 immune-mediated enterocolitis, 86% experienced complete resolution, 3% experienced improvement to Grade 1, and 11% did not improve. Among the 68 patients with Grade 2 enterocolitis, 94% experienced complete resolution, 3% experienced improvement to Grade 1, and 3% did not improve.
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Immune-mediated colitis occurred in 10% (52/547) of patients with RCC and 7% (8/119) of patients with CRC. Median time to onset of immune-mediated colitis was 1.7 months (range: 2 days to 19.2 months) in patients with RCC and 2.4 months (range: 22 days to 5.2 months) in patients with CRC.
Immune-mediated colitis led to permanent discontinuation of YERVOY and nivolumab in 3.2% of patients with RCC or CRC (n=666) and withholding of both YERVOY and nivolumab in 3.9% [see Dosage and Administration (2.5)]. All patients with colitis required systemic corticosteroids, including 80% who received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 21 days (range: 1 day to 27 months). Approximately 23% of patients with immune-mediated colitis required addition of infliximab to high-dose corticosteroids. Complete resolution occurred in 88% of patients. Two patients with RCC had recurrence of colitis after re-initiation of nivolumab with YERVOY.
5.2 Immune-Mediated Hepatitis
Immune-mediated hepatitis, including fatal cases, can occur with YERVOY.
Monitor liver function tests (hepatic transaminase and bilirubin levels) and assess patients for signs and symptoms of hepatotoxicity before each dose of YERVOY. In patients with hepatotoxicity, rule out infectious or malignant causes and increase frequency of liver function test monitoring until resolution.
Permanently discontinue YERVOY in patients with Grade 3 to 4 hepatotoxicity and administer systemic corticosteroids at a dose of 1 to 2 mg/kg/day of prednisone or equivalent. When liver function tests show sustained improvement or return to baseline, initiate corticosteroid tapering and continue to taper over 1 month. Across the clinical development program for YERVOY, mycophenolate treatment has been administered in patients who have persistent severe hepatitis despite high-dose corticosteroids. Withhold YERVOY in patients with Grade 2 hepatotoxicity [see Dosage and Administration (2.5)].
YERVOY as a Single Agent
Metastatic Melanoma
In patients receiving YERVOY 3 mg/kg in MDX010-20, severe, life-threatening, or fatal hepatotoxicity (AST or ALT elevations of more than 5 times the upper limit of normal or total bilirubin elevations more than 3 times the upper limit of normal; Grade 3 to 5) occurred in 8 YERVOY-treated patients (2%), with fatal hepatic failure in 0.2% and hospitalization in 0.4% of YERVOY-treated patients. An additional 13 patients (2.5%) experienced moderate hepatotoxicity manifested by liver function test abnormalities (AST or ALT elevations of more than 2.5 times but not more than 5 times the upper limit of normal or total bilirubin elevation of more than 1.5 times but not more than 3 times the upper limit of normal; Grade 2). The underlying pathology was not ascertained in all patients but in some instances included immune-mediated hepatitis. There were insufficient numbers of patients with biopsy-proven hepatitis to characterize the clinical course of this event.
Adjuvant Treatment of Melanoma
In patients receiving YERVOY 10 mg/kg in CA184-029, Grade 3 to 4 immune-mediated hepatitis occurred in 51 patients (11%) and moderate Grade 2 immune-mediated hepatitis occurred in 22 patients (5%). Liver biopsy performed in 6 patients with Grade 3 to 4 hepatitis showed evidence of toxic or autoimmune hepatitis. The median time to onset for Grade 3 to 4 hepatitis was 2.0 months (range: 1 day to 4.2 months) and for Grade 2 hepatitis was 1.4 months (range: 13 days to 6.5 months). Of the 51 patients with Grade 3 to 4 immune-mediated hepatitis, 94% experienced complete resolution, 4% experienced improvement to Grade 1, and 2% did not improve. Of the 22 patients with Grade 2 immune-mediated hepatitis, 91% experienced complete resolution and 9% did not improve.
Forty-six patients (90%) with Grade 3 to 4 hepatitis were treated with systemic corticosteroids. The median duration of treatment was 4.4 months (ranging up to 56.1 months). Sixteen patients (73%) with moderate hepatitis were treated with systemic corticosteroids. The median duration of treatment was 2.6 months (ranging up to 41.4 months).
Concurrent Administration with Vemurafenib
In a dose-finding trial, Grade 3 increases in transaminases with or without concomitant increases in total bilirubin occurred in 6 of 10 patients who received concurrent YERVOY (3 mg/kg) and vemurafenib (960 mg BID or 720 mg BID).
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Immune-mediated hepatitis occurred in 7% (38/547) of patients with RCC and 8% (10/119) with CRC. Median time to onset was 2 months (range: 14 days to 26.8 months) in patients with RCC and 2.2 months (range: 22 days to 10.5 months) in patients with CRC.
Immune-mediated hepatitis led to permanent discontinuation of YERVOY and nivolumab in 3.6% of patients with RCC or CRC (n=666) and withholding of both YERVOY and nivolumab in 3.5% [see Dosage and Administration (2.5)]. All patients with hepatitis required systemic corticosteroids, including 94% who received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 1 month (range: 1 day to 7 months). Approximately 19% of patients with immune-mediated hepatitis required addition of mycophenolic acid to high-dose corticosteroids. Complete resolution occurred in 83% of patients. No patients had recurrence of hepatitis after re-initiation of nivolumab with YERVOY or nivolumab alone.
5.3 Immune-Mediated Dermatitis/Skin Adverse Reactions
Immune-mediated dermatitis, including fatal cases, can occur with YERVOY.
Monitor patients for signs and symptoms of dermatitis, such as rash and pruritus. Unless an alternate etiology has been identified, signs or symptoms of dermatitis should be considered immune-mediated.
Permanently discontinue YERVOY in patients with Stevens-Johnson syndrome, toxic epidermal necrolysis, or rash complicated by full thickness dermal ulceration, or necrotic, bullous, or hemorrhagic manifestations. Administer systemic corticosteroids at a dose of 1 to 2 mg/kg/day of prednisone or equivalent. When dermatitis is controlled, corticosteroid tapering should occur over a period of at least 1 month. Withhold YERVOY dosing in patients with moderate to severe signs and symptoms [see Dosage and Administration (2.5)].
For mild to moderate dermatitis, such as localized rash and pruritus, treat symptomatically. Administer topical or systemic corticosteroids if there is no improvement of symptoms within 1 week.
YERVOY as a Single Agent
Metastatic Melanoma
In patients receiving YERVOY 3 mg/kg in MDX010-20, severe, life-threatening, or fatal immune-mediated dermatitis (e.g., Stevens-Johnson syndrome, toxic epidermal necrolysis, or rash complicated by full thickness dermal ulceration, or necrotic, bullous, or hemorrhagic manifestations; Grade 3 to 5) occurred in 13 YERVOY-treated patients (2.5%). One patient (0.2%) died as a result of toxic epidermal necrolysis and one additional patient required hospitalization for severe dermatitis. There were 63 patients (12%) with moderate (Grade 2) dermatitis.
The median time to onset of moderate, severe, or life-threatening immune-mediated dermatitis was 22 days and ranged up to 4.0 months from the initiation of YERVOY.
Seven YERVOY-treated patients (54%) with severe dermatitis received high-dose corticosteroids (median dose 60 mg prednisone/day or equivalent) for up to 3.4 months followed by corticosteroid taper. Of these 7 patients, 6 had complete resolution; time to resolution ranged up to 3.6 months.
Of the 63 patients with moderate dermatitis, 25 (40%) were treated with systemic corticosteroids (median of 60 mg/day of prednisone or equivalent) for a median of 15 days, 7 (11%) were treated with only topical corticosteroids, and 31 (49%) did not receive systemic or topical corticosteroids. Forty-four patients (70%) with moderate dermatitis were reported to have complete resolution, 7 (11%) improved to mild (Grade 1) severity, and 12 (19%) had no reported improvement.
Adjuvant Treatment of Melanoma
In patients receiving YERVOY 10 mg/kg in CA184-029, Grade 3 to 4 immune-mediated dermatitis occurred in 19 patients (4%). There were 99 patients (21%) with moderate (Grade 2) dermatitis. The median time to onset for Grade 3 to 4 dermatitis was 14 days (range: 5 days to 11.3 months) and for Grade 2 dermatitis was 11 days (range: 1 day to 16.6 months).
Sixteen patients (84%) with Grade 3 to 4 dermatitis were treated with systemic corticosteroids for a median of 21 days (ranging up to 49.2 months) resulting in complete resolution of dermatitis within a median time of 4.3 months (range up to 44.4 months). Of the 3 patients (16%) not treated with systemic or topical corticosteroids, 2 (11%) had complete resolution and 1 had improvement to Grade 1.
Of the 99 patients with Grade 2 dermatitis, 67 (68%) were treated with systemic corticosteroids for a median of 2.6 months, 16 (16%) were treated with only topical corticosteroids and 16 (16%) did not receive systemic or topical corticosteroids. Seventy-seven patients (78%) had complete resolution, 15 (15%) improved to mild (Grade 1) severity, and 7 (7%) did not improve.
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Immune-mediated rash occurred in 16% (90/547) of patients with RCC and 14% (17/119) of patients with CRC. Median time to onset was 1.5 months (range: 1 day to 20.9 months) in RCC and 26 days (range: 5 days to 9.8 months) in CRC.
Immune-mediated rash led to permanent discontinuation or withholding of YERVOY and nivolumab in 0.5% of patients with RCC or CRC (n=666) and withholding of YERVOY and nivolumab in 2.6% of patients [see Dosage and Administration (2.5)]. All patients with immune-mediated rash required systemic corticosteroids, including 19% who received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 22 days (range: 1 day to 23 months). Complete resolution occurred in 66% of patients. Immune-mediated rash recurred in approximately 3% (3/98) of patients who resumed nivolumab.
5.4 Immune-Mediated Neuropathies
Immune-mediated neuropathies, including fatal cases, can occur with YERVOY.
Monitor for symptoms of motor or sensory neuropathy such as unilateral or bilateral weakness, sensory alterations, or paresthesia. Permanently discontinue YERVOY in patients with severe neuropathy (interfering with daily activities) such as Guillain-Barré-like syndromes. Institute medical intervention as appropriate for management of severe neuropathy. Consider initiation of systemic corticosteroids at a dose of 1 to 2 mg/kg/day prednisone or equivalent for severe neuropathies. Withhold YERVOY dosing in patients with moderate neuropathy (not interfering with daily activities) [see Dosage and Administration (2.5)].
YERVOY as a Single Agent
Metastatic Melanoma
In patients receiving YERVOY 3 mg/kg in MDX010-20, 1 case of fatal Guillain-Barré syndrome and 1 case of severe (Grade 3) peripheral motor neuropathy were reported. Across the clinical development program of YERVOY, myasthenia gravis and additional cases of Guillain-Barré syndrome have been reported.
Adjuvant Treatment of Melanoma
In patients receiving YERVOY 10 mg/kg in CA184-029, Grade 3 to 5 immune-mediated neuropathy occurred in 8 patients (2%); the sole fatality was due to complications of Guillain-Barré syndrome [see Adverse Reactions (6.1)]. Moderate Grade 2 immune-mediated neuropathy occurred in 1 patient (0.2%).
The time to onset across the 9 patients with Grade 2 to 5 immune-mediated neuropathy ranged from 1.4 to 27.4 months. All 8 patients with Grade 3 to 5 neuropathy were treated with systemic corticosteroids (range: 3 days to 38.3 months) and 3 also received tacrolimus. Four of the 8 patients with Grade 3 to 5 immune-mediated neuropathy experienced complete resolution, 1 improved to Grade 1, and 3 did not improve. The single patient with Grade 2 immune-mediated neuropathy experienced complete resolution without the use of corticosteroids.
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Among 547 RCC patients, there were 3 cases of Grade 3 paresthesia/hypoesthesia.
5.5 Immune-Mediated Endocrinopathies
Immune-mediated endocrinopathies, including life-threatening cases, can occur with YERVOY.
Monitor patients for clinical signs and symptoms of hypophysitis, adrenal insufficiency (including adrenal crisis), and hyper- or hypothyroidism. Patients may present with fatigue, headache, mental status changes, abdominal pain, unusual bowel habits, and hypotension, or nonspecific symptoms which may resemble other causes such as brain metastasis or underlying disease. Unless an alternate etiology has been identified, signs or symptoms of endocrinopathies should be considered immune-mediated.
Monitor clinical chemistries, adrenocorticotropic hormone (ACTH) level, and thyroid function tests at the start of treatment, before each dose, and as clinically indicated based on symptoms. In a limited number of patients, hypophysitis was diagnosed by imaging studies through enlargement of the pituitary gland.
Withhold YERVOY dosing in symptomatic patients and consider referral to an endocrinologist. Initiate systemic corticosteroids at a dose of 1 to 2 mg/kg/day of prednisone or equivalent, and initiate appropriate hormone replacement therapy [see Dosage and Administration (2.5)].
YERVOY as a Single Agent
Metastatic Melanoma
In patients receiving YERVOY 3 mg/kg in MDX010-20, severe to life-threatening immune-mediated endocrinopathies (requiring hospitalization, urgent medical intervention, or interfering with activities of daily living; Grade 3 to 4) occurred in 9 YERVOY-treated patients (1.8%). All 9 patients had hypopituitarism and some had additional concomitant endocrinopathies such as adrenal insufficiency, hypogonadism, and hypothyroidism. Six of the 9 patients were hospitalized for severe endocrinopathies. Moderate endocrinopathy (requiring hormone replacement or medical intervention; Grade 2) occurred in 12 patients (2.3%) and consisted of hypothyroidism, adrenal insufficiency, hypopituitarism, and 1 case each of hyperthyroidism and Cushing’s syndrome. The median time to onset of moderate to severe immune-mediated endocrinopathy was 2.5 months and ranged up to 4.4 months after the initiation of YERVOY.
Of the 21 patients with moderate to life-threatening endocrinopathy, 17 patients required long-term hormone replacement therapy including, most commonly, adrenal hormones (n=10) and thyroid hormones (n=13).
Adjuvant Treatment of Melanoma
In patients receiving YERVOY 10 mg/kg in CA184-029, Grade 3 to 4 immune-mediated endocrinopathies occurred in 39 patients (8%) and Grade 2 immune-mediated endocrinopathies in 93 patients (20%). Of the 39 patients with Grade 3 to 4 immune-mediated endocrinopathies, 35 patients had hypopituitarism (associated with one or more secondary endocrinopathies, e.g., adrenal insufficiency, hypogonadism, and hypothyroidism), 3 patients had hyperthyroidism, and 1 had primary hypothyroidism. The median time to onset of Grade 3 to 4 immune-mediated endocrinopathy was 2.2 months (range: 2 days to 8 months). Twenty-seven of the 39 patients (69%) were hospitalized for immune-mediated endocrinopathies, and 4 patients (10%) were reported to have resolution.
Of the 93 patients with Grade 2 immune-mediated endocrinopathy, 74 had primary hypopituitarism (associated with one or more secondary endocrinopathy, e.g., adrenal insufficiency, hypogonadism, and hypothyroidism), 9 had primary hypothyroidism, 3 had hyperthyroidism, 3 had thyroiditis with hypo- or hyperthyroidism, 2 had hypogonadism, 1 had both hyperthyroidism and hypopituitarism, and 1 subject developed Graves’ ophthalmopathy. The median time to onset of Grade 2 immune-mediated endocrinopathy was 2.1 months (range: 9 days to 19.3 months), and 20% were reported to have resolution.
One hundred twenty-four patients received systemic corticosteroids as immunosuppression and/or adrenal hormone replacement for Grade 2 to 4 immune-mediated endocrinopathy. Of these, 42 (34%) were able to discontinue corticosteroids. Seventy-three patients received thyroid hormones for treatment of Grade 2 to 4 immune-mediated hypothyroidism. Of these, 14 patients (19%) were able to discontinue thyroid replacement therapy.
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Hypophysitis. Hypophysitis occurred in 4.6% (25/547) of patients with RCC and 3.4% (4/119) of patients with CRC. Median time to onset was 2.8 months (range: 1.3 months to 7.3 months) in patients with RCC and 3.7 months (range: 2.8 to 5.5 months) in patients with CRC.
Hypophysitis led to permanent discontinuation or withholding of YERVOY and nivolumab in 1.2% and 2.6% of patients with RCC or CRC (n=666), respectively [see Dosage and Administration (2.5)]. Approximately 72% of patients with hypophysitis received hormone replacement therapy and 55% received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 13 days (range: 1 day to 1.6 months).
Adrenal Insufficiency. Adrenal insufficiency occurred in 7% (41/547) of patients with RCC and 5.9% (7/119) patients with CRC. Median time to onset was 3.4 months (range: 2.0 months to 22.3 months) in RCC and 3.7 months (range: 2.5 to 13.4 months) in CRC.
Adrenal insufficiency led to permanent discontinuation of YERVOY and nivolumab in 1.2% of patients with RCC or CRC (n=666) and withholding of YERVOY and nivolumab in 2.6% [see Dosage and Administration (2.5)]. Approximately 94% of patients with adrenal insufficiency received hormone replacement therapy and 27% received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 12 days (range: 2 days to 5.6 months).
Hypothyroidism and Hyperthyroidism. Hypothyroidism or thyroiditis resulting in hypothyroidism occurred in 22% (119/547) of patients with RCC and 15% (18/119) of patients with CRC. Median time to onset was 2.2 months (range: 1 day to 21.4 months) in patients with RCC and 2.3 months (range: 22 days to 9.8 months) in patients with CRC. Of the 137 patients with RCC or CRC who developed hypothyroidism, approximately 81% of patients with RCC and 78% with CRC received levothyroxine.
Hyperthyroidism occurred in 12% (66/547) of patients with RCC and 12% (14/119) of patients with CRC. Median time to onset was 1.4 months (range: 6 days to 14.2 months) in RCC and 1.1 months (range: 21 days to 5.4 months) in CRC. Of the 80 patients with RCC or CRC who developed hyperthyroidism, approximately 15% received methimazole and 2% received carbimazole.
Type 1 Diabetes Mellitus. Diabetes occurred in 2.7% (15/547) of patients with RCC. Median time to onset was 3.2 months (range: 19 days to 16.8 months). Both YERVOY and nivolumab were withheld in 33% of patients and both were permanently discontinued in 20% of patients who developed diabetes [see Dosage and Administration (2.5)].
5.6 Immune-Mediated Pneumonitis
Immune-mediated pneumonitis, including fatal cases, can occur with nivolumab with YERVOY. Monitor patients for signs with radiographic imaging and for symptoms of pneumonitis. Administer corticosteroids at a dose of 1 to 2 mg/kg/day prednisone equivalents for moderate (Grade 2) or more severe (Grade 3-4) pneumonitis, followed by corticosteroid taper. Withhold YERVOY dosing in patients with moderate to severe signs and symptoms. Permanently discontinue YERVOY for life-threatening (Grade 4) pneumonitis [see Dosage and Administration (2.5)].
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Immune-mediated pneumonitis occurred in 4.4% (24/547) of patients with RCC and 1.7% (2/119) of patients with CRC. Median time to onset of immune-mediated pneumonitis was 2.6 months (range: 8 days to 9.2 months) in patients with RCC and 1.9 months (range: 27 days to 3 months) in patients with CRC.
Immune-mediated pneumonitis led to permanent discontinuation of YERVOY and nivolumab in 1.8% of patients with RCC or CRC (n=666) and withholding of YERVOY and nivolumab in 1.7% [see Dosage and Administration (2.5)]. All patients with pneumonitis required systemic corticosteroids, including 92% who received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 19 days (range: 4 days to 3.2 months). Approximately 8% required addition of infliximab to high-dose corticosteroids. Complete resolution of pneumonitis occurred in 81% of patients.
5.7 Immune-Mediated Nephritis and Renal Dysfunction
Immune-mediated nephritis can occur with nivolumab with YERVOY. Monitor patients for elevated serum creatinine prior to and periodically during treatment. Administer corticosteroids at a dose of 1 to 2 mg/kg/day prednisone equivalents followed by corticosteroid taper for life-threatening (Grade 4) increased serum creatinine. Administer corticosteroids at a dose of 0.5 to 1 mg/kg/day prednisone equivalents for moderate (Grade 2) or severe (Grade 3) increased serum creatinine, if worsening or no improvement occurs, increase dose of corticosteroids to 1 to 2 mg/kg/day prednisone equivalents. Withhold YERVOY dosing in patients with moderate to severe signs and symptoms. Permanently discontinue YERVOY for life-threatening (Grade 4) increased serum creatinine [see Dosage and Administration (2.5)].
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Immune-mediated nephritis and renal dysfunction occurred in 4.6% (25/547) of patients with RCC and 1.7% (2/119) of patients with CRC. Median time to onset was 3 months (range: 1 day to 13.2 months) among these 27 patients.
Immune-mediated nephritis and renal dysfunction led to permanent discontinuation of YERVOY and nivolumab in 1.2% of patients with RCC or CRC (n=666) and withholding of nivolumab and YERVOY in 2.3% of patients with RCC or CRC [see Dosage and Administration (2.5)]. Approximately 78% of patients with immune-mediated nephritis and renal dysfunction received high-dose corticosteroids (at least 40 mg prednisone equivalents per day) for a median duration of 17 days (range: 1 day to 6 months). Complete resolution occurred in 63% of patients.
5.8 Immune-Mediated Encephalitis
Immune-mediated encephalitis can occur with YERVOY. Evaluation of patients with neurologic symptoms may include, but not be limited to, consultation with a neurologist, brain MRI, and lumbar puncture.
Withhold YERVOY in patients with new-onset moderate to severe neurologic signs or symptoms and evaluate to rule out infectious or other causes of moderate to severe neurologic deterioration. If other etiologies are ruled out, administer corticosteroids at a dose of 1 to 2 mg/kg/day prednisone equivalents for patients with immune-mediated encephalitis, followed by corticosteroid taper. Permanently discontinue YERVOY for immune-mediated encephalitis [see Dosage and Administration (2.5)].
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Encephalitis occurred in one patient (0.2%) with RCC approximately 4 months after initiation of YERVOY and in one patient (0.8%) with CRC 15 days after initiation of YERVOY. The patient with CRC required infliximab and high-dose corticosteroids (at least 40 mg prednisone equivalents per day).
5.9 Infusion Reactions
Severe infusion reactions can occur with nivolumab with YERVOY. Discontinue YERVOY in patients with severe or life-threatening infusion reactions. Interrupt or slow the rate of infusion in patients with mild or moderate infusion reactions [see Dosage and Administration (2.5)].
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
Infusion-related reactions occurred in 5.1% (28/547) of patients with RCC and 4.2% (5/119) of patients with CRC.
5.10 Other Immune-Mediated Adverse Reactions
YERVOY as a Single Agent
Permanently discontinue YERVOY for clinically significant or severe immune-mediated adverse reactions. Initiate systemic corticosteroids at a dose of 1 to 2 mg/kg/day prednisone or equivalent for severe immune-mediated adverse reactions.
Monitor patients for signs or symptoms of ocular toxicity, which may include blurred vision and reduced visual acuity. Immune-mediated ocular toxicity may be associated with retinal detachment or permanent vision loss. Administer corticosteroid eye drops to patients who develop uveitis, iritis, or episcleritis. Permanently discontinue YERVOY for immune-mediated ocular disease that is unresponsive to local immunosuppressive therapy [see Dosage and Administration (2.5)]. If uveitis occurs in combination with other immune-mediated adverse reactions, consider a Vogt-Koyanagi-Harada-like syndrome, which has been observed in patients receiving YERVOY and may require treatment with systemic steroids to reduce the risk of permanent vision loss.
Fatal or serious graft-versus-host disease (GVHD) can occur in patients who receive a CTLA-4 receptor blocking antibody either before or after allogeneic hematopoietic stem cell transplantation (HSCT). Follow patients closely for evidence of GVHD and intervene promptly. [See Adverse Reactions (6.2).] Consider the benefit versus risks of treatment with a CTLA-4 receptor blocking antibody after allogeneic HSCT.
Metastatic Melanoma
In MDX010-20, the following clinically significant immune-mediated adverse reactions were seen in less than 1% of YERVOY-treated patients: cytopenias, nephritis, pneumonitis, meningitis, pericarditis, uveitis, and iritis.
Adjuvant Treatment of Melanoma
In CA184-029, the following clinically significant immune-mediated adverse reactions were seen in less than 1% of YERVOY-treated patients unless specified: cytopenias, eosinophilia (2.1%), pancreatitis (1.3%), meningitis, pneumonitis, sarcoidosis, pericarditis, uveitis, and fatal myocarditis [see Adverse Reactions (6.1)].
Other Clinical Experience
Across 21 dose-ranging trials administering YERVOY at doses of 0.1 to 20 mg/kg (n=2478), the following likely immune-mediated adverse reactions were also reported with less than 1% incidence unless specified: angiopathy, temporal arteritis, vasculitis, polymyalgia rheumatica, conjunctivitis, blepharitis, episcleritis, scleritis, iritis, leukocytoclastic vasculitis, erythema multiforme, psoriasis, arthritis, autoimmune thyroiditis, neurosensory hypoacusis, autoimmune central neuropathy (encephalitis), myositis, polymyositis, ocular myositis, cytopenias (2.5%), and nephritis.
YERVOY 1 mg/kg administered with nivolumab 3 mg/kg
YERVOY can cause other clinically significant and potentially fatal immune-mediated adverse reactions. Immune-mediated adverse reactions may occur after discontinuation of YERVOY therapy. For any suspected immune-mediated adverse reactions, exclude other causes. Based on the severity of the adverse reaction, permanently discontinue or withhold YERVOY, administer high-dose corticosteroids, and if appropriate, initiate hormone-replacement therapy. Upon improvement to Grade 1 or less, initiate corticosteroid taper and continue to taper over at least 1 month. Consider restarting YERVOY after completion of corticosteroid taper based on the severity of the event.
Across clinical trials of YERVOY administered with nivolumab or in trials of nivolumab administered as a single agent, the following clinically significant immune-mediated adverse reactions, some with fatal outcome, occurred in less than 1.0% of patients: myocarditis, rhabdomyolysis, myositis, uveitis, iritis, pancreatitis, facial and abducens nerve paresis, demyelination, polymyalgia rheumatica, autoimmune neuropathy, Guillain-Barré syndrome, hypopituitarism, systemic inflammatory response syndrome, gastritis, duodenitis, sarcoidosis, histiocytic necrotizing lymphadenitis (Kikuchi lymphadenitis), motor dysfunction, vasculitis, aplastic anemia, pericarditis, and myasthenic syndrome.
5.11 Embryo-Fetal Toxicity
Based on its mechanism of action and data from animal studies, YERVOY can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, administration of ipilimumab to cynomolgus monkeys from the onset of organogenesis through delivery resulted in higher incidences of abortion, stillbirth, premature delivery (with corresponding lower birth weight), and higher incidences of infant mortality in a dose-related manner. The effects of ipilimumab are likely to be greater during the second and third trimesters of pregnancy. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with a YERVOY-containing regimen and for 3 months after the last dose of YERVOY [see Use in Specific Populations (8.1, 8.3)].
5.12 Risks Associated When Administered in Combination with Nivolumab
When YERVOY is administered in combination with nivolumab, refer to the nivolumab prescribing information for additional risk information that applies to the combination use.
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling.
• Immune-mediated enterocolitis/colitis [see Warnings and Precautions (5.1)].
• Immune-mediated hepatitis [see Warnings and Precautions (5.2)].
• Immune-mediated dermatitis/skin adverse reactions [see Warnings and Precautions (5.3)].
• Immune-mediated neuropathies [see Warnings and Precautions (5.4)].
• Immune-mediated endocrinopathies [see Warnings and Precautions (5.5)].
• Immune-mediated pneumonitis [see Warnings and Precautions (5.6)].
• Immune-mediated nephritis and renal dysfunction [see Warnings and Precautions (5.7)].
• Immune-mediated encephalitis [see Warnings and Precautions (5.8)].
• Infusion reactions [see Warnings and Precautions (5.9)].
• Other immune-mediated adverse reactions [see Warnings and Precautions (5.10)].
• Embryo-fetal toxicity [see Warnings and Precautions (5.11)].
In patients receiving YERVOY 3 mg/kg for unresectable or metastatic melanoma in MDX010-20, 15% of patients receiving monotherapy and 12% of patients treated in combination with gp100 peptide vaccine experienced Grade 3 to 5 immune-mediated reactions. In patients receiving YERVOY 10 mg/kg for adjuvant treatment of melanoma in CA184-029, 41% experienced Grade 3 to 5 immune-mediated reactions.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed cannot be directly compared with rates in other clinical trials or experience with therapeutics in the same class and may not reflect the rates observed in clinical practice.
The data described below reflect exposure to YERVOY 3 mg/kg as a single agent in MDX010-20, a randomized trial in patients with unresectable or metastatic melanoma; to YERVOY 10 mg/kg as a single agent in CA184-029, a randomized trial in patients with resected Stage IIIA (>1 mm nodal involvement), IIIB, and IIIC (with no in-transit metastases) cutaneous melanoma; and to YERVOY 1 mg/kg, administered in combination with nivolumab, in two trials: CHECKMATE-214 (NCT02231749), a randomized trial in previously untreated patients with advanced renal cell carcinoma, and CHECKMATE-142 (NCT02060188), an open-label, multicenter, non-randomized multiple parallel cohort trial in patients with previously treated, MSI-H or dMMR metastatic colorectal cancer.
Clinically significant adverse reactions were evaluated in a total of 982 patients treated in MDX010-20 and CA184-029 and in 21 dose-ranging trials (n=2478) administering YERVOY at doses of 0.1 to 20 mg/kg [see Warnings and Precautions (5.6)].
Unresectable or Metastatic Melanoma
The safety of YERVOY was evaluated in MDX010-20, a randomized, double-blind clinical trial in which 643 previously treated patients with unresectable or metastatic melanoma received YERVOY 3 mg/kg for 4 doses given by intravenous infusion as a single agent (n=131), YERVOY with an investigational gp100 peptide vaccine (gp100) (n=380), or gp100 peptide vaccine as a single agent (n=132) [see Clinical Studies (14.1)]. Patients in the trial received a median of 4 doses (range: 1 to 4 doses).
MDX010-20 excluded patients with active autoimmune disease or those receiving systemic immunosuppression for organ transplantation.
The trial population characteristics were: median age 57 years (range: 19 to 90), 59% male, 94% white, and baseline ECOG performance status 0 (56%).
YERVOY was discontinued for adverse reactions in 10% of patients.
Table 2 presents selected adverse reactions from MDX010-20, which occurred in at least 5% of patients in the YERVOY-containing arms and with at least 5% increased incidence over the control gp100 arm for all-grade events and at least 1% incidence over the control group for Grade 3 to 5 events.
Table 2: Selected Adverse Reactions in MDX010-20
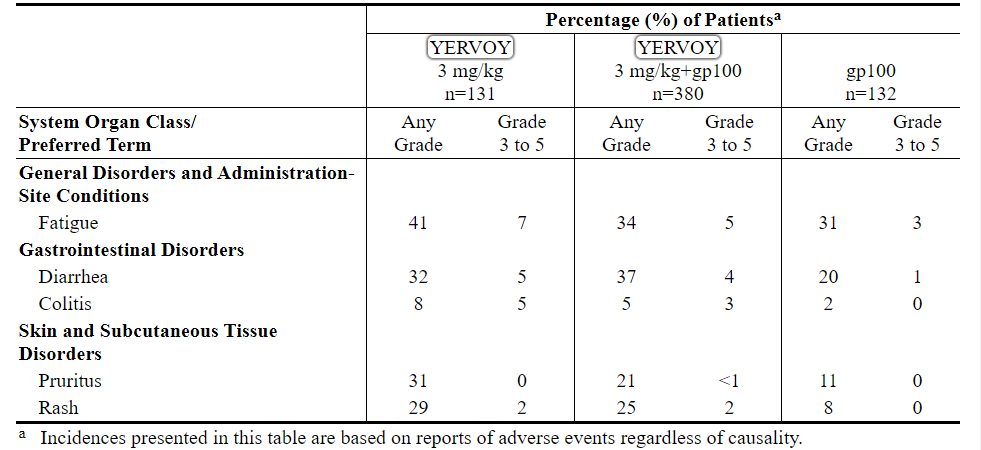
Table 3 presents the per-patient incidence of severe, life-threatening, or fatal immune-mediated adverse reactions from MDX010-20.
Table 3: Severe to Fatal Immune-Mediated Adverse Reactions in MDX010-20
Adjuvant Treatment of Melanoma
The safety of YERVOY was evaluated in CA184-029, a randomized (1:1), double-blind, placebo-controlled trial in which 945 patients with resected Stage IIIA (>1 mm nodal involvement), IIIB, and IIIC (with no in-transit metastases) cutaneous melanoma received YERVOY 10 mg/kg (n=471) or placebo (n=474) administered as an intravenous infusion for 4 doses every 3 weeks followed by 10 mg/kg every 12 weeks beginning at Week 24 up to a maximum of 3 years [see Clinical Studies (14.2)]. In this trial, 36% of patients received YERVOY for longer than 6 months and 26% of patients received YERVOY for longer than 1 year. YERVOY-treated patients in the trial received a median of 4 doses (range: 1 to 16).
CA184-029 excluded patients with prior systemic therapy for melanoma, autoimmune disease, a condition requiring systemic immunosuppression, or a positive test for hepatitis B, hepatitis C, or HIV.
The trial population characteristics were: median age 51 years (range: 18 to 84 years), 62% male, 99% white, and baseline ECOG performance status 0 (94%).
YERVOY was discontinued for adverse reactions in 52% of patients.
Table 4 presents selected adverse reactions from CA184-029 which occurred in at least 5% of YERVOY-treated patients and with at least 5% increased incidence over the placebo group for all-grade events.
Table 4: Selected Adverse Reactions in CA184-029
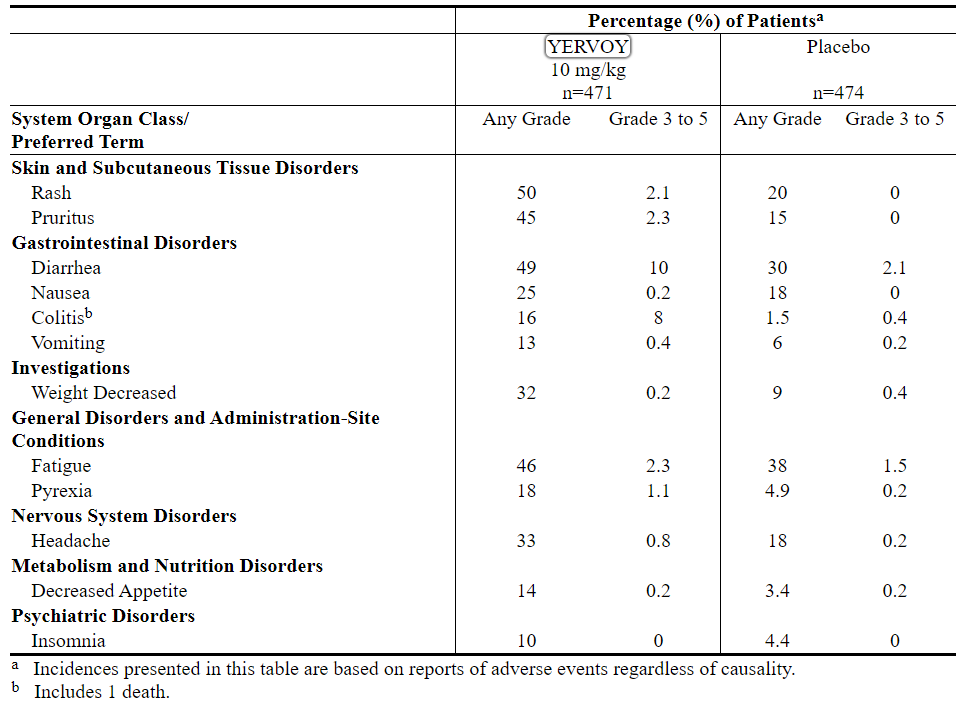
Table 5 presents selected laboratory abnormalities from CA184-029 which occurred in at least 10% of YERVOY-treated patients at a higher incidence compared to placebo.
Table 5: Laboratory Abnormalities Worsening from Baseline Occurring in ≥10% of YERVOY-Treated Patients (CA184-029)a
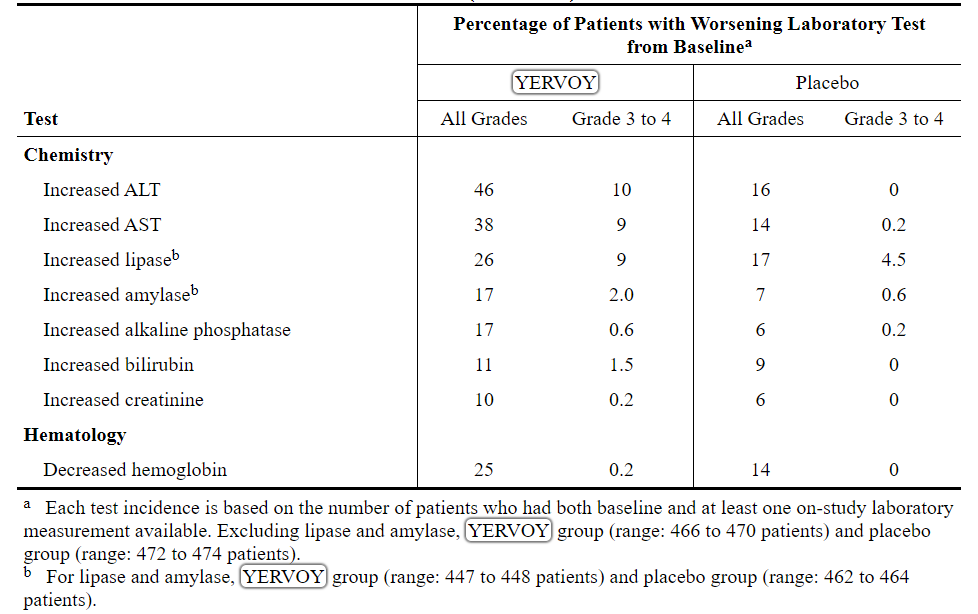
Table 6 presents the per-patient incidence of severe, life-threatening, or fatal immune-mediated adverse reactions from CA184-029.
Table 6: Severe to Fatal Immune-Mediated Adverse Reactions in CA184-029
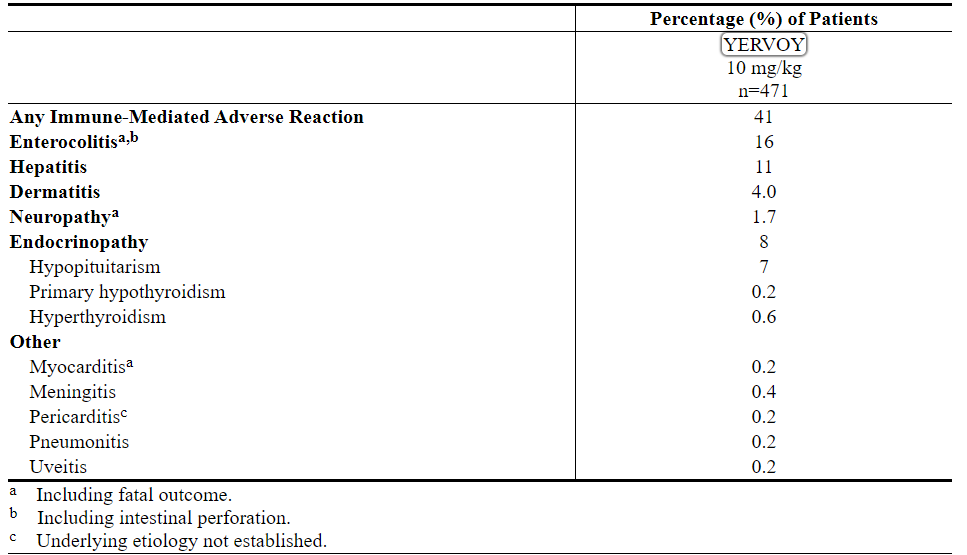
Other Clinical Experience
Across clinical studies that utilized YERVOY doses ranging from 0.3 to 10 mg/kg, the following adverse reactions were also reported (incidence less than 1% unless otherwise noted): urticaria (2%), large intestinal ulcer, esophagitis, acute respiratory distress syndrome, renal failure, and infusion reaction.
Previously Untreated Renal Cell Carcinoma
The safety of nivolumab 3 mg/kg, administered with YERVOY 1 mg/kg was evaluated in CHECKMATE-214, a randomized open-label trial in which 1082 patients with previously untreated advanced RCC received nivolumab 3 mg/kg in combination with YERVOY 1 mg/kg every 3 weeks for 4 doses followed by nivolumab monotherapy at the 3 mg/kg dose (n=547) every 2 weeks or sunitinib administered orally 50 mg daily for 4 weeks followed by 2 weeks off, every cycle (n=535) [see Clinical Studies (14.3)]. The median duration of treatment was 7.9 months (range: 1 day to 21.4+ months) in nivolumab plus YERVOY-treated patients and 7.8 months (range: 1 day to 20.2+ months) in sunitinib-treated patients. In this trial, 57% of patients in the nivolumab plus YERVOY arm were exposed to treatment for greater than 6 months, and 38% of patients were exposed to treatment for greater than 1 year.
Study therapy was discontinued for adverse reactions in 31% of nivolumab plus YERVOY patients and in 21% of sunitinib patients. Fifty-four percent (54%) of patients receiving nivolumab plus YERVOY and 43% of patients receiving sunitinib had a drug delay for an adverse reaction. In the sunitinib group, 53% of patients required a dose reduction; dose reductions were not permitted in the nivolumab plus YERVOY treatment group. Serious adverse reactions occurred in 59% of patients receiving nivolumab plus YERVOY and in 43% of patients receiving sunitinib. The most frequent serious adverse reactions reported in at least 2% of patients treated with nivolumab plus YERVOY were diarrhea, pyrexia, pneumonia, pneumonitis, hypophysitis, acute kidney injury, dyspnea, adrenal insufficiency, and colitis; in patients treated with sunitinib, they were pneumonia, pleural effusion, and dyspnea.
The most common adverse reactions (reported in at least 20% of nivolumab plus YERVOY-treated patients) were fatigue, rash, diarrhea, musculoskeletal pain, pruritus, nausea, cough, pyrexia, arthralgia, vomiting, dyspnea, and decreased appetite. Table 7 summarizes adverse reactions that occurred in greater than 15% of nivolumab plus YERVOY-treated patients.
Table 7: Grade 1-4 Adverse Reactions in >15% of Patients Receiving Nivolumab plus YERVOY (CHECKMATE-214)
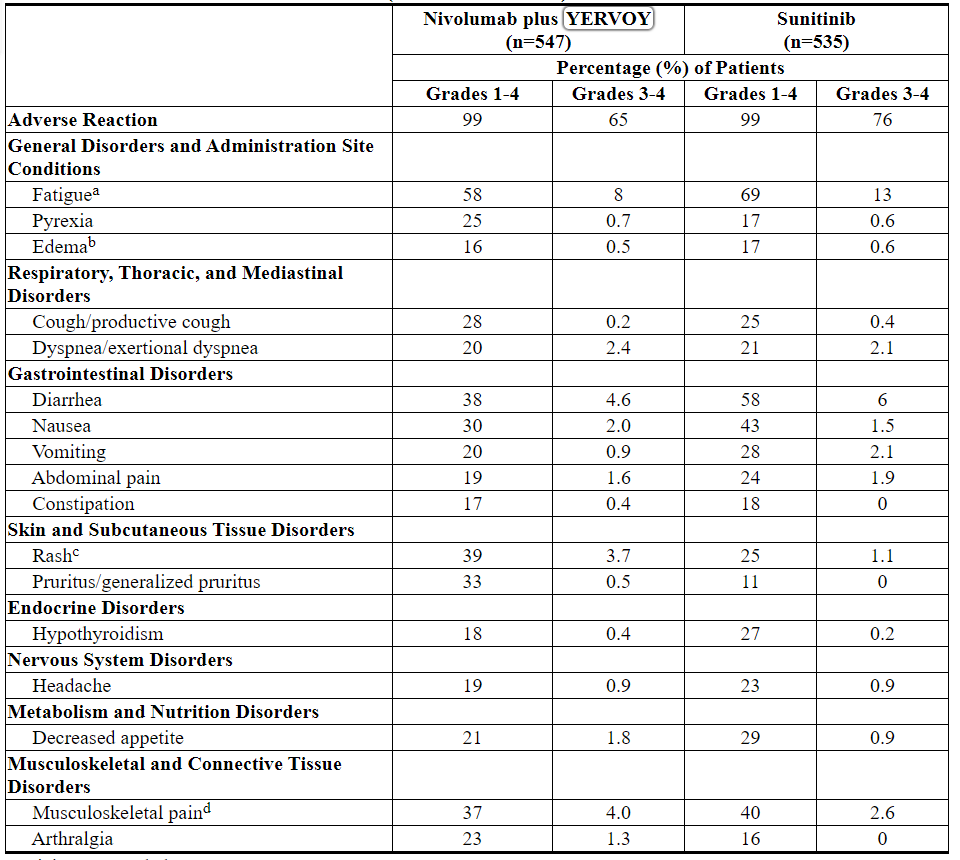

The most common laboratory abnormalities which have worsened compared to baseline in ≥30% of nivolumab plus YERVOY-treated patients include increased lipase, anemia, increased creatinine, increased ALT, increased AST, hyponatremia, increased amylase, and lymphopenia. Table 8 summarizes the laboratory abnormalities that occurred in greater than 15% of nivolumab plus YERVOY-treated patients.
Table 8: Grade 1-4 Laboratory Values Worsening from Baseline Occurring in >15% of Patients on Nivolumab plus YERVOY (CHECKMATE-214)
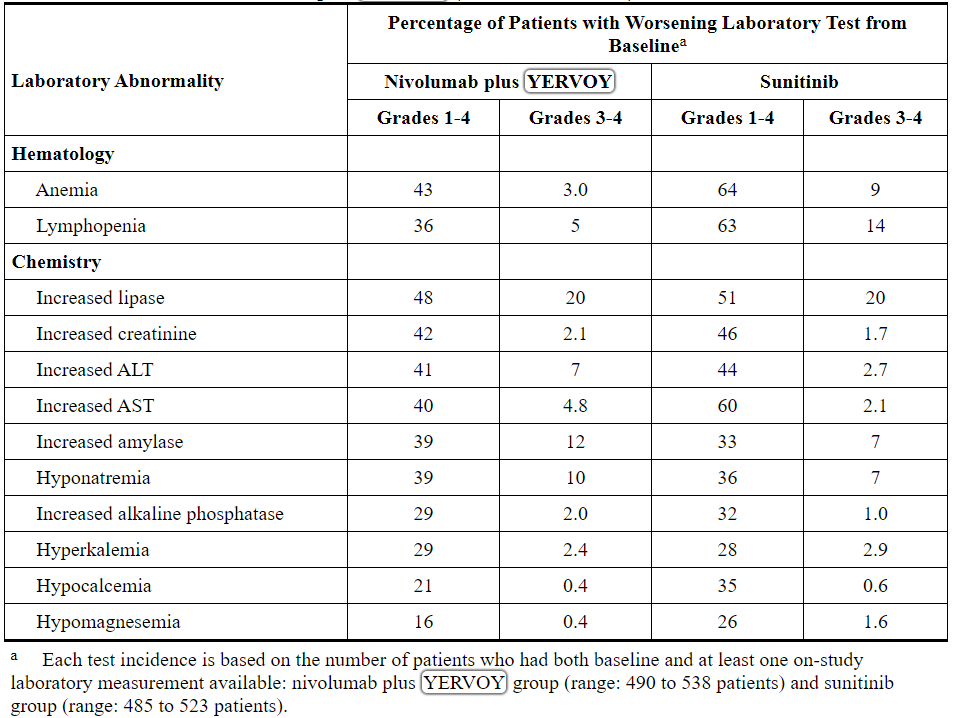
In addition, among patients with TSH less than or equal to the ULN at baseline, a lower proportion of patients experienced a treatment-emergent elevation of TSH greater than the ULN in the nivolumab plus YERVOY group compared to the sunitinib group (31% and 61%, respectively).
Previously Treated MSI-H or dMMR Metastatic Colorectal Cancer
The safety of YERVOY was evaluated in CHECKMATE-142, an open-label, multicenter, non-randomized, multiple parallel-cohort study. In CHECKMATE-142, 119 patients with previously treated MSI-H or dMMR mCRC received YERVOY, in combination with nivolumab, in a single-arm cohort. In another single-arm cohort under CHECKMATE-142, 74 patients with mCRC received nivolumab monotherapy. All patients in both cohorts had received prior fluorouracil-based chemotherapy for metastatic disease. Of those in the YERVOY plus nivolumab cohort, 69% had received prior treatment with a fluoropyrimidine, oxaliplatin, and irinotecan, and 29% had received an anti-EGFR antibody.
Patients in the YERVOY plus nivolumab cohort received YERVOY 1 mg/kg and nivolumab 3 mg/kg on Day 1 of each 21-day cycle for 4 doses, then nivolumab 3 mg/kg every 2 weeks until disease progression or unacceptable toxicity. Patients in the nivolumab single agent cohort received nivolumab 3 mg/kg every 3 weeks until disease progression or unacceptable toxicity [See Clinical Studies (14.4)].
The median duration of exposure for YERVOY was 2.1 months. Serious adverse reactions occurred in 47% of YERVOY-treated patients. The most frequent serious adverse reactions reported in at least 2% of patients were colitis/diarrhea, hepatic events, abdominal pain, acute kidney injury, pyrexia, and dehydration. The most common adverse reactions (reported in at least 20% of YERVOY-treated patients) were fatigue, diarrhea, pyrexia, musculoskeletal pain, abdominal pain, pruritus, nausea, rash, decreased appetite, and vomiting.
Table 9 summarizes adverse reactions that occurred in greater than 10% of patients receiving YERVOY. Table 10 summarizes laboratory tests that worsened from baseline in greater than 10% of patients receiving YERVOY. Based on the design of CHECKMATE-142, the data summarized below cannot be used to identify statistically significant differences between the two cohorts for any adverse reaction.
Table 9: Adverse Reactions Occurring in ≥10% of Patients (CHECKMATE-142)
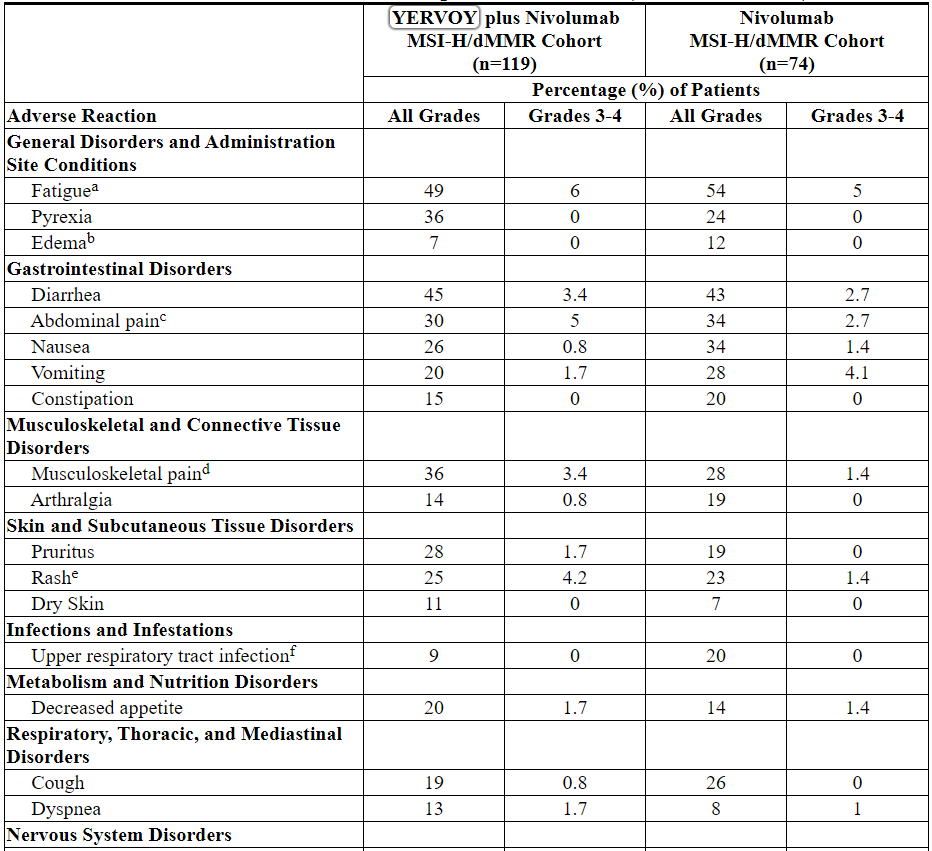

Other clinically important adverse reactions reported in less than 10% of patients receiving YERVOY in CHECKMATE-142 were encephalitis (0.8%), necrotizing myositis (0.8%), and uveitis (0.8%).
Table 10: Laboratory Abnormalities Worsening from Baseline Occurring in ≥10% of Patients (CHECKMATE-142)

6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of YERVOY. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune system disorders: graft-versus-host disease
Skin and Subcutaneous Tissue Disorders: Drug reaction with eosinophilia and systemic symptoms (DRESS syndrome)
6.3 Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to ipilimumab in the studies described below with the incidences of antibodies in other studies or to other products may be misleading.
Eleven (1.1%) of 1024 evaluable patients with unresectable or metastatic melanoma tested positive for treatment-emergent binding antibodies against ipilimumab (TE-ADAs) in an electrochemiluminescent (ECL) based assay. This assay had substantial limitations in detecting anti-ipilimumab antibodies in the presence of ipilimumab. Seven (4.9%) of 144 patients receiving ipilimumab and 7 (4.5%) of 156 patients receiving placebo for the adjuvant treatment of melanoma tested positive for TE-ADAs using an ECL assay with improved drug tolerance. No patients tested positive for neutralizing antibodies. No infusion-related reactions occurred in patients who tested positive for TE-ADAs.
Of 499 patients evaluable for anti-ipilimumab antibodies in CHECKMATE-214 and CHECKMATE-142, 27 (5.4%) were positive for anti-ipilimumab antibodies; there were no patients with neutralizing antibodies against ipilimumab. There was no evidence of increased incidence of infusion reactions to YERVOY in patients with anti-ipilimumab antibodies. Of 503 patients evaluable for anti-nivolumab antibodies in CHECKMATE-214 and CHECKMATE-142 trials, 126 (25%) were positive for anti-nivolumab antibodies and 3 (0.6%) were positive for neutralizing antibodies against nivolumab.
7 DRUG INTERACTIONS
No formal pharmacokinetic drug interaction studies have been conducted with YERVOY.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on data from animal studies and its mechanism of action, YERVOY can cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. In animal reproduction studies, administration of ipilimumab to cynomolgus monkeys from the onset of organogenesis through delivery resulted in higher incidences of abortion, stillbirth, premature delivery (with corresponding lower birth weight), and higher incidences of infant mortality in a dose-related manner (see Data). The effects of ipilimumab are likely to be greater during the second and third trimesters of pregnancy. Human IgG1 is known to cross the placental barrier and ipilimumab is an IgG1; therefore, ipilimumab has the potential to be transmitted from the mother to the developing fetus. There is insufficient human data for YERVOY exposure in pregnant women. Advise pregnant women of the potential risk to a fetus.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
A Pregnancy Safety Surveillance Study has been established to collect information about pregnancies in women who have received YERVOY. Healthcare providers are encouraged to enroll patients or have their patients enroll directly by calling 1-844-593-7869.
Data
Animal Data
In a combined study of embryo-fetal and peri-postnatal development, pregnant cynomolgus monkeys received ipilimumab every 3 weeks from the onset of organogenesis in the first trimester through parturition. No treatment-related adverse effects on reproduction were detected during the first two trimesters of pregnancy. Beginning in the third trimester, administration of ipilimumab at doses resulting in exposures approximately 2.6 to 7.2 times the human exposure at a dose of 3 mg/kg resulted in dose-related increases in abortion, stillbirth, premature delivery (with corresponding lower birth weight), and an increased incidence of infant mortality. In addition, developmental abnormalities were identified in the urogenital system of 2 infant monkeys exposed in utero to 30 mg/kg of ipilimumab (7.2 times the AUC in humans at the 3 mg/kg dose). One female infant monkey had unilateral renal agenesis of the left kidney and ureter, and 1 male infant monkey had an imperforate urethra with associated urinary obstruction and subcutaneous scrotal edema.
Genetically engineered mice heterozygous for CTLA-4 (CTLA-4+/−), the target for ipilimumab, appeared healthy and gave birth to healthy CTLA-4+/− heterozygous offspring. Mated CTLA-4+/− heterozygous mice also produced offspring deficient in CTLA-4 (homozygous negative, CTLA-4−/−). The CTLA-4−/− homozygous negative offspring appeared healthy at birth, exhibited signs of multiorgan lymphoproliferative disease by 2 weeks of age, and all died by 3 to 4 weeks of age with massive lymphoproliferation and multiorgan tissue destruction.
8.2 Lactation
Risk Summary
It is not known whether YERVOY is present in human milk. In monkeys, ipilimumab was present in milk (see Data). There are no data to assess the effects of YERVOY on milk production. Advise women to discontinue breastfeeding during treatment with YERVOY and for 3 months following the final dose.
Data
In monkeys treated at dose levels resulting in exposures 2.6 and 7.2 times higher than those in humans at a 3 mg/kg dose, ipilimumab was present in milk at concentrations of 0.1 mcg/mL and 0.4 mcg/mL, representing a ratio of up to 0.3% of the steady-state serum concentration of the drug.
8.3 Females and Males of Reproductive Potential
Contraception
Based on its mechanism of action, YERVOY can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)]. Advise females of reproductive potential to use effective contraception during treatment with YERVOY and for 3 months following the last dose of YERVOY.
8.4 Pediatric Use
The safety and effectiveness of YERVOY have been established in pediatric patients 12 years and older for the treatment of unresectable or metastatic melanoma or for the treatment of microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan. Use of YERVOY in this age group is supported by evidence from adequate and well-controlled studies of YERVOY in adults and population pharmacokinetic data demonstrating that the exposure at doses of 3 mg/kg and 1 mg/kg in the pediatric and adult populations are comparable. In addition, the tumor biology and course of advanced melanoma and MSI-H or dMMR metastatic colorectal cancer are sufficiently similar in adults and pediatric patients 12 years and older to allow extrapolation of data from adults to pediatric patients.
The safety and effectiveness for pediatric patients 12 years and older have not been established for the adjuvant treatment of melanoma or for the treatment of renal cell carcinoma. In addition, the safety and effectiveness have not been established with YERVOY for any indication in pediatric patients less than 12 years of age.
YERVOY was evaluated in a total of 45 pediatric patients across two clinical trials. In a dose-finding trial, 33 pediatric patients with relapsed or refractory solid tumors were evaluated. The median age was 13 years (range 2 to 21 years), and 20 patients were ≥12 years old. YERVOY was administered at doses of 1, 3, 5, and 10 mg/kg intravenously over 90 minutes every 3 weeks for 4 doses and then every 12 weeks thereafter until progression or treatment discontinuation.
YERVOY was also evaluated in an open-label, single-arm trial in 12 pediatric patients ≥12 years old (range 12 to 16 years) with previously treated or untreated, unresectable Stage 3 or 4 malignant melanoma. Patients received YERVOY 3 mg/kg (4 patients) or 10 mg/kg (8 patients) intravenously over 90 minutes every 3 weeks for 4 doses.
Of the 17 patients ≥12 years of age with melanoma treated with YERVOY across both studies, two patients experienced objective responses including one partial response that was sustained for 16 months. There were no responses in patients with non-melanoma solid tumors.
The overall safety profile of YERVOY in children and adolescents was consistent with the safety profile in adults.
Pediatric Pharmacokinetics (PK)
Based on a population PK analysis using available pooled data from 565 patients from four phase 2 adult studies (N=521) and two pediatric studies (N=44), body weight normalized clearance of ipilimumab is comparable between adult and pediatric patients. In pediatric patients with a dosing regimen of 3 mg/kg every 3 weeks, the model simulated geometric mean (CV%) steady-state serum peak and trough concentrations of ipilimumab were 65.8 (17.6%) and 20.7 (33.1%) mcg/mL (for 2 to 6 years old), 70.1 (19.6%) and 19.6 (42.9%) mcg/mL (for 6 to <12 years old), and 73.3 (20.6%) and 17.8 (50.8%) mcg/mL (for 12 years and older), which are comparable to those in adult patients.
8.5 Geriatric Use
Of the 511 patients treated with YERVOY in MDX010-20 (unresectable or metastatic melanoma), 28% were 65 years and over. No overall differences in safety or efficacy were reported between the elderly patients (65 years and over) and younger patients (less than 65 years).
CA184-029 (adjuvant treatment of melanoma) and CHECKMATE-142 (metastatic colorectal cancer) did not include sufficient numbers of patients aged 65 years and older to determine whether they respond differently from younger patients.
Of the 550 patients randomized to nivolumab 3 mg/kg administered with YERVOY 1 mg/kg in CHECKMATE-214 (renal cell carcinoma), 38% were 65 years or older and 8% were 75 years or older. No overall difference in safety was reported between elderly patients and younger patients. In elderly patients with intermediate or poor risk, no overall difference in effectiveness was reported.
8.6 Renal Impairment
No dose adjustment is needed for patients with renal impairment [see Clinical Pharmacology (12.3)].
8.7 Hepatic Impairment
No dose adjustment is needed for patients with mild hepatic impairment (total bilirubin [TB] >1.0 to 1.5 times the upper limit of normal [ULN] or AST >ULN). YERVOY has not been studied in patients with moderate (TB >1.5 to 3.0 times ULN and any AST) or severe (TB >3 times ULN and any AST) hepatic impairment [see Clinical Pharmacology (12.3)].
10 OVERDOSAGE
There is no information on overdosage with YERVOY.
11 DESCRIPTION
Ipilimumab is a recombinant, human monoclonal antibody that binds to the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4). Ipilimumab is an IgG1 kappa immunoglobulin with an approximate molecular weight of 148 kDa. Ipilimumab is produced in mammalian (Chinese hamster ovary) cell culture.
YERVOY is a sterile, preservative-free, clear to slightly opalescent, colorless to pale-yellow solution for intravenous infusion, which may contain a small amount of visible translucent-to-white, amorphous ipilimumab particulates. It is supplied in single-use vials of 50 mg/10 mL and 200 mg/40 mL. Each milliliter contains 5 mg of ipilimumab and the following inactive ingredients: diethylene triamine pentaacetic acid (DTPA) (0.04 mg), mannitol (10 mg), polysorbate 80 (vegetable origin) (0.1 mg), sodium chloride (5.85 mg), tris hydrochloride (3.15 mg), and Water for Injection, USP at a pH of 7.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
CTLA-4 is a negative regulator of T-cell activity. Ipilimumab is a monoclonal antibody that binds to CTLA-4 and blocks the interaction of CTLA-4 with its ligands, CD80/CD86. Blockade of CTLA-4 has been shown to augment T-cell activation and proliferation, including the activation and proliferation of tumor infiltrating T-effector cells. Inhibition of CTLA-4 signaling can also reduce T-regulatory cell function, which may contribute to a general increase in T cell responsiveness, including the anti-tumor immune response.
12.3 Pharmacokinetics
The pharmacokinetics (PK) of ipilimumab was studied in 785 patients with unresectable or metastatic melanoma who received doses of 0.3, 3, or 10 mg/kg once every 3 weeks for 4 doses. The PK of ipilimumab is linear in the dose range of 0.3 to 10 mg/kg. Following administration of YERVOY every 3 weeks, the systemic accumulation was 1.5-fold or less. Steady-state concentrations of ipilimumab were reached by the third dose; the mean Cmin at steady state was 19.4 mcg/mL at 3 mg/kg and 58.1 mcg/mL at 10 mg/kg every 3 weeks. The mean value (percent coefficient of variation) based on population PK analysis for the terminal half-life (t1/2) was 15.4 days (34%) and for clearance (CL) was 16.8 mL/h (38%).
YERVOY with nivolumab: When YERVOY 1 mg/kg was administered in combination with nivolumab 3 mg/kg, the CL of ipilimumab and nivolumab were unchanged compared to when YERVOY was administered alone.
When administered in combination, the CL of ipilimumab was unchanged in presence of anti-ipilimumab antibodies and the CL of nivolumab increased by 20% in the presence of anti-nivolumab antibodies.
Specific Populations
The effects of various covariates on the PK of ipilimumab were assessed in population PK analyses. The CL of ipilimumab increased with increasing body weight supporting the recommended body weight (mg/kg) based dosing. The following factors had no clinically important effect on the CL of ipilimumab: age (range: 23 to 88 years), sex, performance status, renal impairment, mild hepatic impairment, previous cancer therapy, and baseline lactate dehydrogenase (LDH) levels. The effect of race was not examined due to limited data available in non-Caucasian ethnic groups.
Renal Impairment: The effect of renal impairment on the CL of ipilimumab was evaluated in patients with mild (GFR <90 and ≥60 mL/min/1.73 m2; n=349), moderate (GFR <60 and ≥30 mL/min/1.73 m2; n=82), or severe (GFR <30 and ≥15 mL/min/1.73 m2; n=4) renal impairment compared to patients with normal renal function (GFR ≥90 mL/min/1.73 m2; n=350) in population PK analyses. No clinically important differences in the CL of ipilimumab were found between patients with renal impairment and patients with normal renal function [see Use in Specific Populations (8.6)].
Hepatic Impairment: The effect of hepatic impairment on the CL of ipilimumab was evaluated in patients with mild hepatic impairment (n=76) compared to patients with normal hepatic function (n=708) in the population PK analyses, and no clinically important differences in the CL of ipilimumab were found. YERVOY has not been studied in patients with moderate or severe hepatic impairment [see Use in Specific Populations (8.7)].
Pediatric Population: [see Use in Specific Populations (8.4)].
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
The carcinogenic potential of ipilimumab has not been evaluated in long-term animal studies, and the genotoxic potential of ipilimumab has not been evaluated.
Fertility studies have not been performed with ipilimumab.
14 CLINICAL STUDIES
14.1 Unresectable or Metastatic Melanoma
The safety and efficacy of YERVOY were investigated in a randomized (3:1:1), double-blind, double-dummy trial (MDX010-20, NCT00094653) that included 676 randomized patients with unresectable or metastatic melanoma previously treated with one or more of the following: aldesleukin, dacarbazine, temozolomide, fotemustine, or carboplatin. Of these 676 patients, 403 were randomized to receive YERVOY at 3 mg/kg in combination with an investigational peptide vaccine with incomplete Freund’s adjuvant (gp100), 137 were randomized to receive YERVOY at 3 mg/kg, and 136 were randomized to receive gp100 as a single agent. The trial enrolled only patients with HLA-A2*0201 genotype; this HLA genotype facilitates the immune presentation of the investigational peptide vaccine. The trial excluded patients with active autoimmune disease or those receiving systemic immunosuppression for organ transplantation. YERVOY/placebo was administered at 3 mg/kg as an intravenous infusion every 3 weeks for 4 doses. Gp100/placebo was administered at a dose of 2 mg peptide by deep subcutaneous injection every 3 weeks for 4 doses. Assessment of tumor response was conducted at weeks 12 and 24, and every 3 months thereafter. Patients with evidence of objective tumor response at 12 or 24 weeks had assessment for confirmation of durability of response at 16 or 28 weeks, respectively.
The major efficacy outcome measure was overall survival (OS) in the YERVOY plus gp100 arm compared to that in the single-agent gp100 arm. Secondary efficacy outcome measures were OS in the YERVOY plus gp100 arm compared to the YERVOY arm, OS in the YERVOY arm compared to the gp100 arm, best overall response rate (BORR) at week 24 between each of the trial arms, and duration of response.
Of the randomized patients, 61%, 59%, and 54% in the YERVOY plus gp100, YERVOY, and gp100 arms, respectively, were men. Twenty-nine percent were ≥65 years of age, the median age was 57 years, 71% had M1c stage, 12% had a history of previously treated brain metastasis, 98% had ECOG performance status of 0 and 1, 23% had received aldesleukin, and 38% had elevated LDH level. Sixty-one percent of patients randomized to either YERVOY-containing arm received all 4 planned doses. The median duration of follow-up was 8.9 months.
The OS results are shown in Table 11 and Figure 1.
Table 11: Overall Survival Results
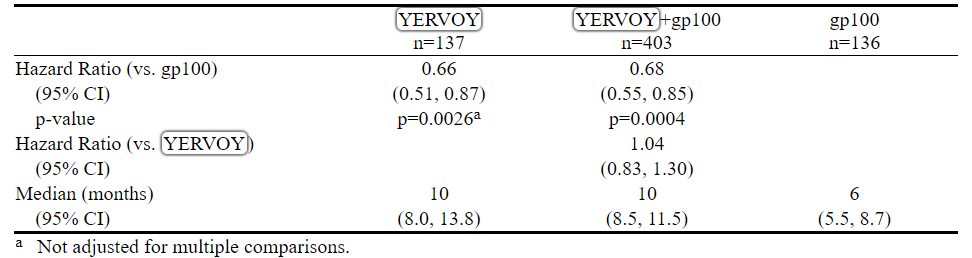
Figure 1: Overall Survival
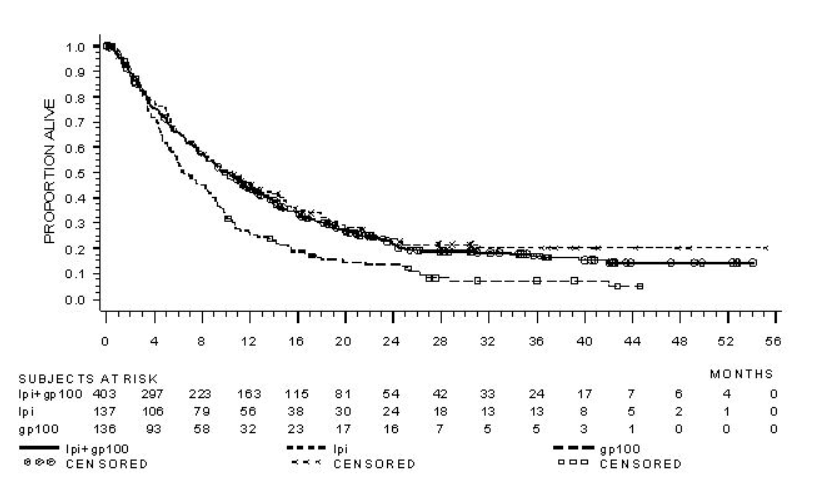
The best overall response rate (BORR) as assessed by the investigator was 5.7% (95% CI: 3.7%, 8.4%) in the YERVOY plus gp100 arm, 10.9% (95% CI: 6.3%, 17.4%) in the YERVOY arm, and 1.5% (95% CI: 0.2%, 5.2%) in the gp100 arm. The median duration of response was 11.5 months in the YERVOY plus gp100 arm and has not been reached in the YERVOY or gp100 arm.
14.2 Adjuvant Treatment of Melanoma
The safety and efficacy of YERVOY for the adjuvant treatment of melanoma were investigated in CA184-029 (NCT00636168), a randomized (1:1), double-blind, placebo-controlled trial in patients with resected Stage IIIA (>1 mm nodal involvement), IIIB, and IIIC (with no in-transit metastases) histologically confirmed cutaneous melanoma. Patients were randomized to receive YERVOY 10 mg/kg or placebo as an intravenous infusion every 3 weeks for 4 doses, followed by YERVOY 10 mg/kg or placebo every 12 weeks from Week 24 to Week 156 (3 years) or until documented disease recurrence or unacceptable toxicity. Enrollment required complete resection of melanoma with full lymphadenectomy within 12 weeks prior to randomization. Patients with prior therapy for melanoma, autoimmune disease, and prior or concomitant use of immunosuppressive agents were ineligible. Randomization was stratified by stage according to American Joint Committee on Cancer (AJCC) 2002 classification (Stage IIIA >1 mm nodal involvement, Stage IIIB, Stage IIIC with 1 to 3 involved lymph nodes, and Stage IIIC with ≥4 involved lymph nodes) and by region (North America, Europe, and Australia). The major efficacy outcome measures were independent review committee (IRC)-assessed recurrence-free survival (RFS), defined as the time between the date of randomization and the earliest date of first recurrence (local, regional, or distant metastasis) or death, and overall survival. Tumor assessment was conducted every 12 weeks for the first 3 years then every 24 weeks until distant recurrence.
Among 951 patients enrolled, 475 were randomized to receive YERVOY and 476 to placebo. Median age was 51 years old (range: 18 to 84), 62% were male, 99% were white, 94% had ECOG performance status of 0. With regard to disease stage, 20% had Stage IIIA with lymph nodes >1 mm, 44% had Stage IIIB, and 36% had Stage IIIC (with no in-transit metastases). Other disease characteristics of the trial population were: clinically palpable lymph nodes (58%), 2 or more positive lymph nodes (54%), and ulcerated primary lesions (42%).
The efficacy results are in Table 12 and in Figure 2.
Table 12: Efficacy Results in CA184-029
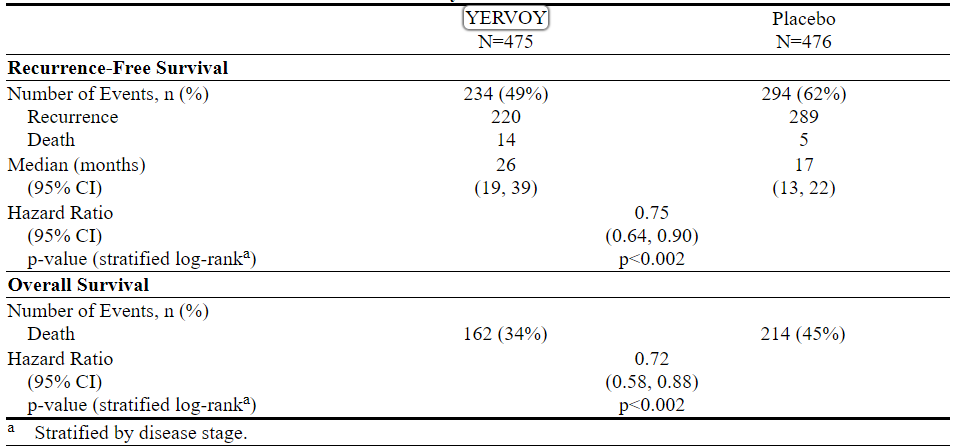
Figure 2: Overall Survival
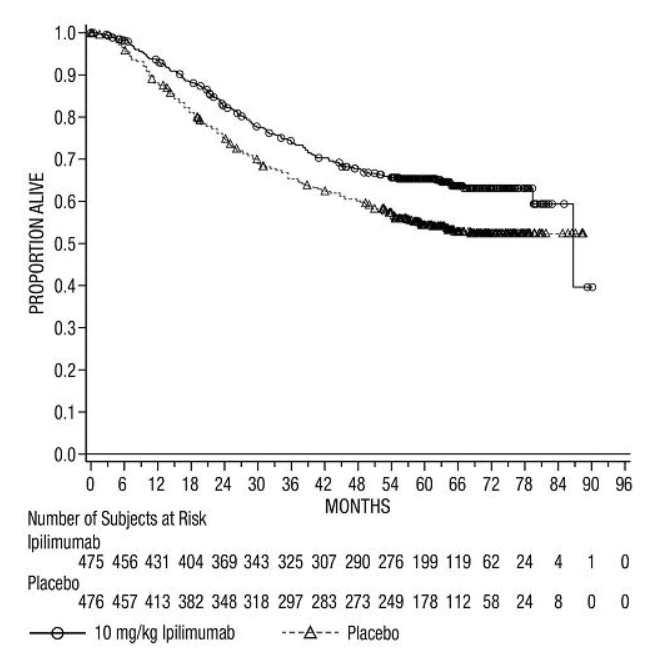
14.3 Previously Untreated Advanced Renal Cell Carcinoma
CHECKMATE-214 (NCT02231749) was a randomized (1:1), open-label study in patients with previously untreated advanced RCC. Patients were included regardless of their PD-L1 status. CHECKMATE-214 excluded patients with any history of or concurrent brain metastases, active autoimmune disease, or medical conditions requiring systemic immunosuppression. Patients were stratified by International Metastatic RCC Database Consortium (IMDC) prognostic score and region.
Efficacy was evaluated in intermediate/poor-risk patients with at least 1 or more of 6 prognostic risk factors as per the IMDC criteria (less than one year from time of initial renal cell carcinoma diagnosis to randomization, Karnofsky performance status <80%, hemoglobin less than the lower limit of normal, corrected calcium of greater than 10 mg/dL, platelet count greater than the upper limit of normal, and absolute neutrophil count greater than the upper limit of normal).
Patients were randomized to nivolumab 3 mg/kg plus YERVOY 1 mg/kg (n=425) administered intravenously every 3 weeks for 4 doses followed by nivolumab monotherapy 3 mg/kg every two weeks or to sunitinib (n=422) administered orally 50 mg daily for 4 weeks followed by 2 weeks off, every cycle. Treatment continued until disease progression or unacceptable toxicity.
The median age was 61 years (range: 21 to 85) with 38% ≥65 years of age and 8% ≥75 years of age. The majority of patients were male (73%) and white (87%) and 26% and 74% of patients had a baseline KPS of 70% to 80% and 90% to 100%, respectively.
The major efficacy outcome measures were OS, PFS (IRRC-assessed), and confirmed ORR (IRRC-assessed) in intermediate/poor-risk patients. In this population, the trial demonstrated statistically significant improvement in OS and ORR for patients randomized to nivolumab plus YERVOY as compared with sunitinib (Table 13 and Figure 3). OS benefit was observed regardless of PD-L1 expression level. The trial did not demonstrate a statistically significant improvement in PFS.
The efficacy results from CHECKMATE-214 are presented in Table 13 and Figure 3.
Table 13: Efficacy Results - CHECKMATE-214
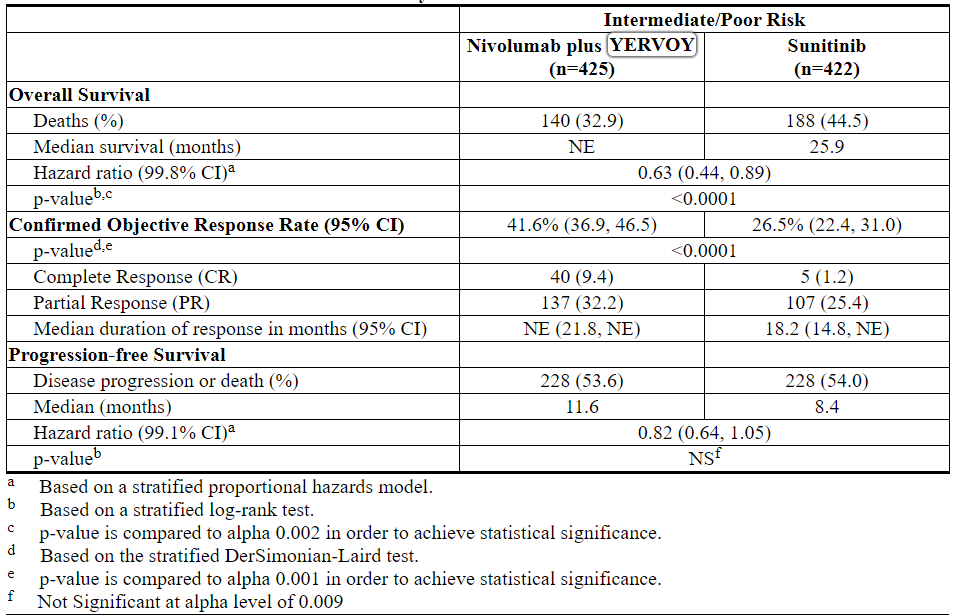
Figure 3: Overall Survival (Intermediate/Poor-Risk Population) - CHECKMATE-214
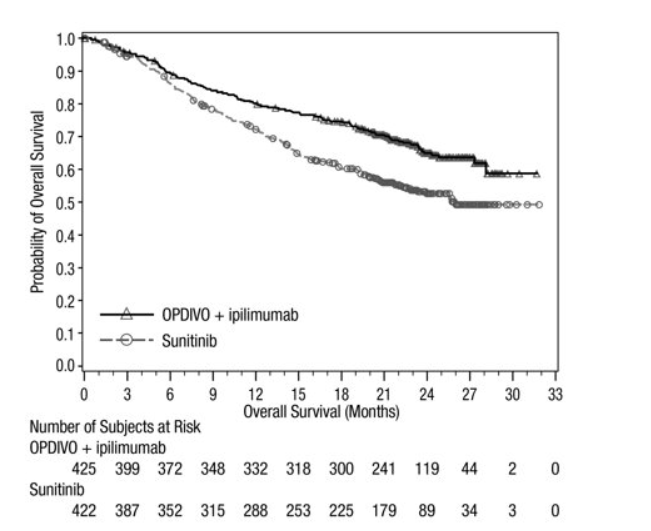
CHECKMATE-214 also randomized 249 favorable risk patients as per IMDC criteria to nivolumab plus YERVOY (n=125) or to sunitinib (n=124). These patients were not evaluated as part of the efficacy analysis population. OS in favorable risk patients receiving nivolumab plus YERVOY compared to sunitinib has a hazard ratio of 1.45 (95% CI: 0.75, 2.81). The efficacy of nivolumab plus YERVOY in previously untreated renal cell carcinoma with favorable risk disease has not been established.
14.4 Microsatellite Instability-High (MSI-H) or Mismatch Repair Deficient (dMMR) Metastatic Colorectal Cancer
CHECKMATE-142 (NCT02060188) was a multicenter, non-randomized, multiple parallel-cohort, open-label study conducted in patients with locally determined dMMR or MSI-H metastatic CRC (mCRC) who had disease progression during or after prior treatment with fluoropyrimidine-, oxaliplatin-, or irinotecan-based chemotherapy. Key eligibility criteria were at least one prior line of treatment for metastatic disease, ECOG PS 0 or 1, and absence of the following: active brain metastases, active autoimmune disease, or medical conditions requiring systemic immunosuppression.
Patients enrolled in the YERVOY and nivolumab MSI-H mCRC cohort received YERVOY 1 mg/kg and nivolumab 3 mg/kg IV every 3 weeks for 4 doses, followed by nivolumab 3 mg/kg IV as a single agent every 2 weeks. Patients enrolled in the single-agent nivolumab MSI-H mCRC cohort received nivolumab 3 mg/kg by intravenous (IV) infusion every 2 weeks. Treatment in both cohorts continued until unacceptable toxicity or radiographic progression.
Tumor assessments were conducted every 6 weeks for the first 24 weeks and every 12 weeks thereafter. Efficacy outcome measures were overall response rate (ORR) as assessed by independent radiographic review committee (IRRC) using Response Evaluation Criteria in Solid Tumors (RECIST v1.1) and duration of response (DOR).
A total of 119 patients were enrolled in the YERVOY plus nivolumab cohort. The median age was 58 years (range: 21 to 88), with 32% ≥65 years of age and 9% ≥75 years of age; 59% were male and 92% were white. Baseline ECOG PS was 0 (45%) or 1 (55%), and 29% were reported to have Lynch Syndrome. Across the cohort, 69% received prior treatment with a fluoropyrimidine, oxaliplatin, and irinotecan; 10%, 40%, 24%, and 15% received 1, 2, 3, or ≥4 prior lines of therapy for metastatic disease, respectively, and 29% had received an anti-EGFR antibody.
A total of 74 patients were enrolled in the single-agent nivolumab cohort. The median age was 53 years (range: 26 to 79) with 23% ≥65 years of age and 5% ≥75 years of age, 59% were male and 88% were white. Baseline ECOG performance status was 0 (43%), 1 (55%), or 3 (1.4%), and 36% were reported to have Lynch Syndrome. Across the 74 patients, 72% received prior treatment with a fluoropyrimidine, oxaliplatin, and irinotecan; 7%, 30%, 28%, 19%, and 16% received 0, 1, 2, 3, or ≥4 prior lines of therapy for metastatic disease, respectively, and 42% of patients had received an anti-EGFR antibody.
Efficacy results are shown in Table 14.
Table 14: Efficacy Results in CHECKMATE-142
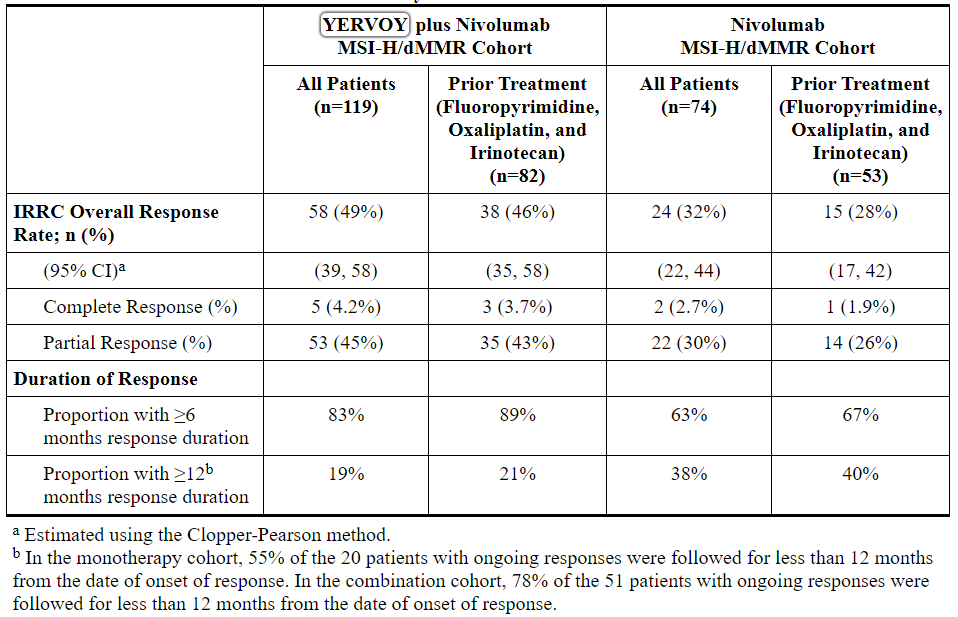
16 HOW SUPPLIED/STORAGE AND HANDLING
YERVOY (ipilimumab) Injection is available as follows:

Store YERVOY under refrigeration at 2°C to 8°C (36°F to 46°F). Protect YERVOY from light by storing in the original carton until time of use. Do not freeze or shake.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Immune-Mediated Adverse Reactions
Inform patients of the risk of immune-mediated adverse reactions that may require corticosteroid treatment and withholding or discontinuation of YERVOY, including:
• Enterocolitis/Colitis: Advise patients to contact their healthcare provider immediately for diarrhea or severe abdominal pain [see Warnings and Precautions (5.1)].
• Hepatitis: Advise patients to contact their healthcare provider immediately for jaundice, severe nausea or vomiting, pain on the right side of abdomen, lethargy, or easy bruising or bleeding [see Warnings and Precautions (5.2)].
• Skin Adverse Reactions: Advise patients to contact their healthcare provider immediately for rash [see Warnings and Precautions (5.3)].
• Neuropathies: Advise patients to contact their healthcare provider immediately for neuropathies [see Warnings and Precautions (5.4)].
• Endocrinopathies: Advise patients to contact their healthcare provider immediately for signs or symptoms of hypophysitis, adrenal insufficiency, hypothyroidism, hyperthyroidism, and diabetes mellitus [see Warnings and Precautions (5.5)].
• Pneumonitis: Advise patients to contact their healthcare provider immediately for any new or worsening cough, chest pain, or shortness of breath [see Warnings and Precautions (5.6)].
• Nephritis and Renal Dysfunction: Advise patients to contact their healthcare provider immediately for signs or symptoms of nephritis including decreased urine output, blood in urine, swelling in ankles, loss of appetite, and any other symptoms of renal dysfunction [see Warnings and Precautions (5.7)].
• Encephalitis: Advise patients to contact their healthcare provider immediately for neurological signs or symptoms of encephalitis [see Warnings and Precautions (5.8)].
Infusion Reactions
• Advise patients of the potential risk of infusion reaction [see Warnings and Precautions (5.9)].
Females of Reproductive Potential
• Advise female patients that YERVOY can cause fetal harm. Advise females of reproductive potential to use effective contraception during treatment with YERVOY and for 3 months after the last dose [see Use in Specific Populations (8.3)].
• Advise female patients to contact their healthcare provider with a known or suspected pregnancy. Advise females who may have been exposed to YERVOY during pregnancy to contact Bristol-Myers Squibb at 1-800-721-5072 [see Warnings and Precautions (5.11) and Use in Specific Populations (8.1, 8.3)]. Advise patients that there is a Pregnancy Safety Surveillance Study that monitors pregnancy outcomes in women exposed to YERVOY during pregnancy, and they can be enrolled by calling 1-844-593-7869 [see Use in Specific Populations (8.1)].
Lactation
• Advise women not to breastfeed during treatment with YERVOY and for 3 months after the last dose [see Use in Specific Populations (8.2)].
Manufactured by:
Bristol-Myers Squibb Company
Princeton, NJ 08543 USA
U.S. License No. 1713[print code]
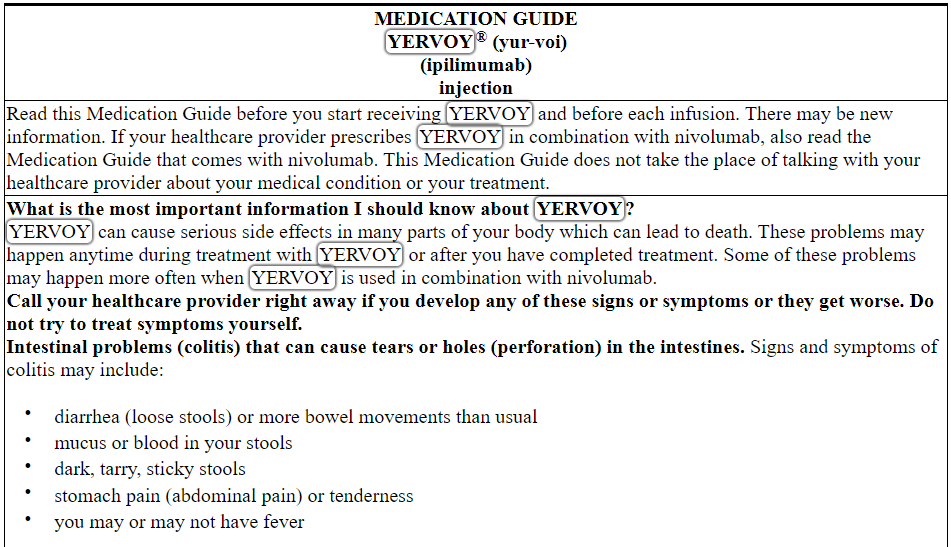
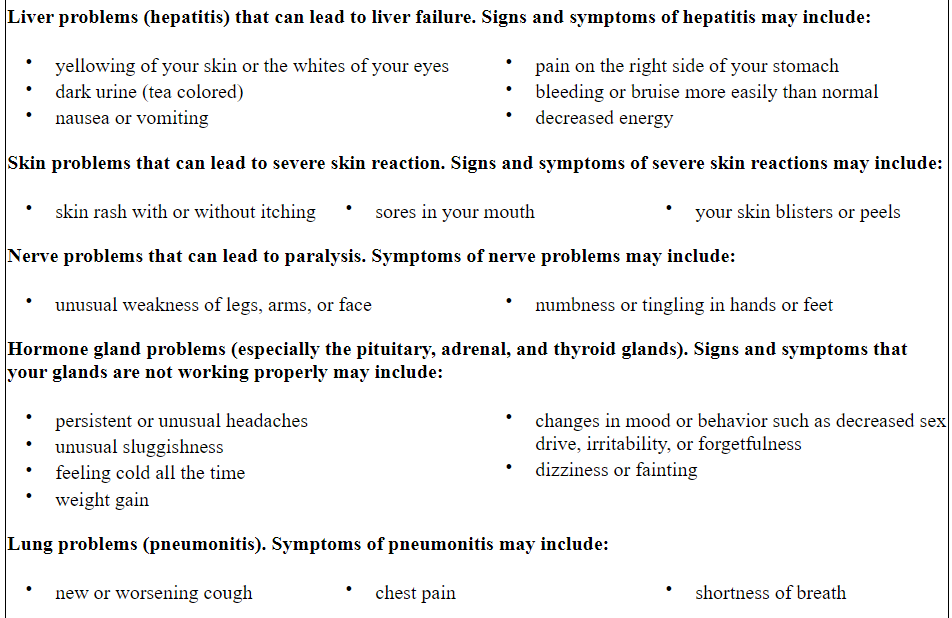

This Medication Guide has been approved by the U.S. Food and Drug Administration.
Revised: May 2019YERVOY 50 mg/10 mL Representative Packaging
See How Supplied section for a complete list of available packages of YERVOY.
NDC 0003-2327-11
Rx only
YERVOY®
(ipilimumab)
Injection
50 mg/10 mL
(5 mg/mL)
For Intravenous Infusion Only
Single-use vial; Discard unused portion
DISPENSE ENCLOSED MEDICATION GUIDE TO EACH PATIENT
Bristol-Myers Squibb
YERVOY 200 mg/40 mL Representative Packaging
NDC 0003-2328-22
Rx only
YERVOY®
(ipilimumab)
Injection
200 mg/40 mL
(5 mg/mL)
For Intravenous Infusion Only
Single-use vial; Discard unused portion
DISPENSE ENCLOSED MEDICATION GUIDE TO EACH PATIENT
Bristol-Myers Squibb
【备注】以上内容仅供参考,不作为用药依据,详情请参照药品附带说明书。

