商品详情
返回产品目录商品包装及说明书因厂家更换频繁,如有不符以实物为主
布格替尼片
国际零售参考价:¥**/盒
-
温馨提醒:本说明书仅供参考,最新的说明书详见药品附带的说明书。
完整的处方信息
1适应症和用途
ALUNBRIG用于治疗已发展或不耐受克唑替尼的间变性淋巴瘤激酶(ALK)阳性转移性非小细胞肺癌(NSCLC)患者。根据肿瘤反应率和反应持续时间,该适应症在加速批准下得到批准[见临床研究(14) ]。继续批准该适应症可能要取决于验证性试验中对临床益处的验证和描述。
2用法用量
2.1推荐剂量
ALUNBRIG的推荐剂量为:
前7天每天口服90 mg;
如果在前7天内耐受90 mg,则每天口服一次,将剂量增加至180 mg。
施用ALUNBRIG直至疾病进展或出现不可接受的毒性。
如果ALUNBRIG因不良反应以外的其他原因而中断了14天或更长时间,则应以90 mg的剂量每天一次恢复治疗7天,然后再增加至先前的耐受剂量。
ALUNBRIG可以带或不带食物一起服用。指导患者完整吞服药片。不要压碎或咀嚼药片。
如果错过一剂ALUNBRIG或在服药后出现呕吐,请不要在预定的时间再服用一剂ALUNBRIG。
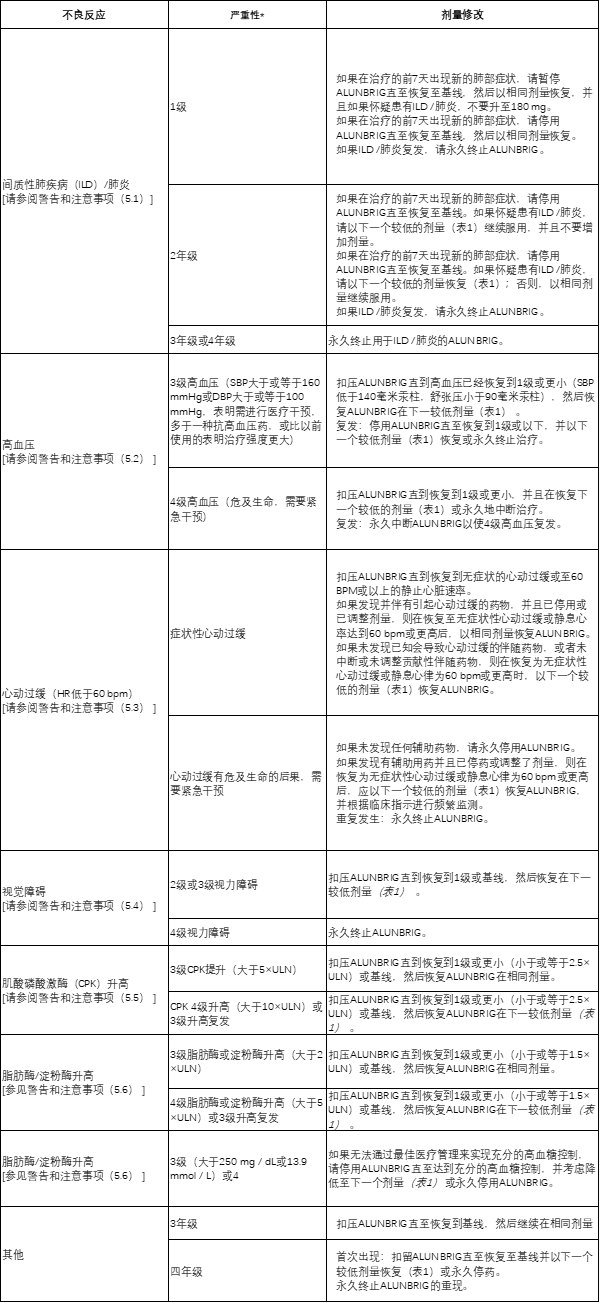
2.2不良反应的剂量修改
表1总结了ALUNBRIG减少不良反应的剂量。

*不适用
一旦减少了不良反应,就不要随后增加ALUNBRIG的剂量。如果患者无法耐受每日一次60 mg的剂量,则永久停用ALUNBRIG。
表2提供了ALUNBRIG用于不良反应管理的剂量修改建议。
2.3强或中度CYP3A抑制剂的剂量修改
在用ALUNBRIG 治疗期间避免同时使用强效或中效 CYP3A抑制剂[见药物相互作用(7.1),临床药理学(12.3) ]。如果不能避免同时使用强效CYP3A抑制剂,则将ALUNBRIG的每日一次剂量减低约50%(即从180 mg减至90 mg,或从90 mg减至60 mg)。如果无法避免中度CYP3A抑制剂的共同给药,则将ALUNBRIG的每日一次剂量减低约40%(即180 mg至120 mg,120 mg至90 mg或90 mg至60 mg)。停用强效或中效 CYP3A抑制剂后,恢复开始CYP3A抑制剂之前耐受的ALUNBRIG剂量。
2.4中度CYP3A诱导剂的剂量修改
在ALUNBRIG 治疗期间避免中度CYP3A诱导剂的共同给药[见药物相互作用(7.1),临床药理学(12.3) ]。如果无法避免中度CYP3A诱导剂的共同给药,则在治疗7天后,以当前的ALUNBRIG耐受剂量增加ALUNBRIG的每日剂量,以30 mg的增量增加一次,最大剂量为开始前耐受的ALUNBRIG剂量的两倍。中度CYP3A诱导剂。
中度CYP3A诱导剂终止后,恢复开始中度CYP3A诱导剂耐受的ALUNBRIG剂量。
2.5重度肝功能不全患者的剂量调整
减少ALUNBRIG约40%,每天一次剂量(即,从180毫克至120毫克,120毫克至90毫克,或90毫克至60毫克)的患者有严重肝损伤(Child-Pugh分级C)[见用途,具体人口(8.6),临床药理学(12.3) ]。
2.6重度肾功能不全患者的剂量调整
对于严重肾功能不全的患者[Cockcroft-Gault肌酐清除率(CLcr)15至29 mL / min],将每日一次ALUNBRIG降低约50%(即从180 mg至90 mg,或从90 mg至60 mg)[参见在特定人群中使用(8.7),临床药理学(12.3) ]。
3剂型和强度
180 mg:椭圆形,白色至类白色薄膜衣片,一侧凹陷有“ U13”,另一侧凹陷
90 mg:椭圆形,白色至类白色薄膜衣片,一侧凹陷有“ U7”,另一侧凹陷
30毫克:圆形,白色至灰白色薄膜衣片,一侧凹陷有“ U3”,另一侧凹陷
4禁忌症
没有。
5警告和注意事项
5.1间质性肺疾病(ILD)/肺炎
ALUNBRIG已发生与间质性肺疾病(ILD)/肺炎一致的严重,危及生命的致命肺不良反应。
在试验性ALTA(ALTA)中,90 mg组(每天90 mg一次)中有3.7%的患者发生ILD /肺炎,而90→180 mg组(180 mg每天一次中有7天铅治疗)的ILD /肺炎发生率是9.1%。每天一次90毫克)。
6.4%的患者较早(在开始ALUNBRIG的 9天之内;中位发作为2天)发生了与可能的ILD /肺炎相一致的不良反应,其中2.7%发生了3至4级反应。
监测是否有新的或恶化的呼吸道症状(例如呼吸困难,咳嗽等),尤其是在开始ALUNBRIG的第一周。对于任何有新的或恶化的呼吸道症状的患者,应停用ALUNBRIG,并立即评估ILD /肺炎或其他呼吸道症状的原因(例如,肺栓塞,肿瘤进展和传染性肺炎)。对于1级或2级ILD /肺炎,恢复到基线后可按照表1降低剂量恢复ALUNBRIG或永久终止ALUNBRIG。对于3级或4级ILD /肺炎或1级或2级ILD /肺炎的复发,永久停用ALUNBRIG [请参阅剂量和用法(2.2),不良反应(6.1) ]。
5.2高血压
在ALTA中,据报道在90 mg组接受ALUNBRIG的患者中有11%患有高血压,在90→180 mg组中有21%的患者中有高血压。总体上有5.9%的患者发生3级高血压。
在使用ALUNBRIG治疗之前控制血压。使用ALUNBRIG治疗2周后,至少每月监测一次血压。扣压ALUNBRIG 3级高血压尽管最佳的降压治疗。解决或改善为1级严重性后,以减少的剂量恢复ALUNBRIG。考虑永久停止使用ALUNBRIG治疗4级高血压或3级高血压复发[请参阅剂量和用法(2.2),不良反应(6.1) ]。
将ALUNBRIG与引起心动过缓的降压药联合使用时,请务必小心[见警告和注意事项(5.3) ]。
5.3心动过缓
心律失常可与ALUNBRIG发生。在ALTA中,90 mg组的5.7%的患者和90→180 mg组的7.6%的患者的心率低于每分钟50次跳动(bpm)。90 mg组中1例(0.9%)患者发生2级心动过缓。
使用ALUNBRIG监测心率和血压。如果无法避免同时使用已知会导致心动过缓的药物,则应更频繁地监测患者[参见警告和注意事项(5.2) ]。
对于有症状的心动过缓,应停用ALUNBRIG并复查已知引起心动过缓的药物。如果发现并伴有引起心动过缓的药物,并且已停药或调整了剂量,则在症状性心动过缓消失后,以相同剂量恢复ALUNBRIG;否则,请在症状性心动过缓消失后减少ALUNBRIG的剂量。如果未发现任何有帮助的伴随用药,请停止使用ALUNBRIG进行危及生命的心动过缓[请参见剂量和用法(2.2) ]。
5.4视觉障碍
在ALTA中,在90 mg组中,接受ALUNBRIG治疗的患者中有7.3%发生了导致视力障碍的不良反应,包括视力模糊,复视和视力下降,在90→180 mg组中,有10%的患者接受了ALUNBRIG治疗。在90→180 mg组中,每1名患者发生3级黄斑水肿和白内障。
劝告患者报告任何视觉症状。扣压ALUNBRIG并获得患者的眼科用评价2级或更大的严重性新的或恶化的视觉症状。将2级或3级视觉障碍恢复至1级严重度或基线后,以减少的剂量恢复ALUNBRIG。永久停止使用ALUNBRIG进行4级视力障碍的治疗[请参阅剂量和用法(2.2),不良反应(6.1) ]。
5.5肌酸磷酸激酶(CPK)升高
在ALTA中,90 mg组中接受ALUNBRIG的患者中有27%发生了肌酸磷酸激酶(CPK)升高,而90 mg→180 mg组中有48%的患者发生了肌酸磷酸激酶(CPK)升高。90 mg组3-4级CPK升高的发生率为2.8%,90→180 mg组为12%。
在90 mg组中,有1.8%的患者降低了CPK剂量,在90→180 mg组中,有4.5%的患者降低了CPK。
劝告患者报告任何无法解释的肌肉疼痛,压痛或无力。在ALUNBRIG治疗期间监控CPK水平。扣压ALUNBRIG为3或4级CPK升高。拆分或恢复至1级或基线后,以表2中所述的相同剂量或降低剂量恢复ALUNBRIG [请参阅剂量和用法(2.2),不良反应(6.1) ]。
5.6胰酶升高
在ALTA中,90 mg组中27%的患者和90→180 mg组中39%的患者发生淀粉酶升高。90 mg组中21%的患者和90→180 mg组中45%的患者出现脂肪酶升高。90 mg组的患者中有3.7%的患者发生3或4级淀粉酶升高,而90→180 mg组的患者中有2.7%的患者发生了3级或4级淀粉酶升高。90 mg组的患者中有4.6%的患者发生3或4级脂肪酶升高,而90→180 mg组的患者中发生了5.5%的患者。
用ALUNBRIG治疗期间监测脂肪酶和淀粉酶。扣压ALUNBRIG为3或4级胰酶升高。解决或恢复至1级或基线后,以表2中所述的相同剂量或降低剂量恢复ALUNBRIG [请参阅剂量和用法(2.2),不良反应(6.1) ]。
5.7高血糖
在ALTA中,接受ALUNBRIG的患者中有43%经历了新的或恶化的高血糖症。根据实验室对血清空腹血糖水平的评估,3级高血糖发生在3.7%的患者中。在基线时有20名糖尿病或葡萄糖耐受不良的20名患者中,有2名(10%)在接受ALUNBRIG时需要开始胰岛素治疗。
在开始ALUNBRIG之前评估空腹血糖,此后定期监测。根据需要启动或优化降血糖药物。如果无法通过最佳医疗管理来实现充分的降血糖控制,请停用ALUNBRIG直至达到充分的降血糖控制,并考虑按照表1所述减少ALUNBRIG的剂量或永久停用ALUNBRIG [请参阅剂量和给药方法(2.2),不良反应(6.1) ]。
5.8胚胎-胎儿毒性
根据其作用机制和在动物中的发现,对孕妇服用ALUNBRIG会引起胎儿伤害。没有关于孕妇使用ALUNBRIG的临床数据。在器官发生期间向怀孕的大鼠施用brigatinib导致剂量相关的骨骼异常,剂量低至12.5 mg / kg /天(约为180毫克AUC每天一次的人暴露量的0.7倍),并且在术后增加-每天25 mg / kg /天的剂量(大约是人类每天180 mg暴露量的1.26倍)时,植入物的丢失,畸形和胎儿体重降低。
建议妇女注意胎儿的潜在危险。建议有生殖潜力的女性在使用ALUNBRIG治疗期间以及最终剂量后至少4个月内使用有效的非激素避孕方法。提醒男性生殖潜在的治疗过程中使用的有效避孕的女性伴侣和的最后一次给药后至少3个月ALUNBRIG [见特殊人群中使用(8.1,8.3) ,临床药理学(12.1) ]。
6不良反应
在处方信息的其他部分,将更详细地讨论以下不良反应:
间质性肺疾病(ILD)/肺炎[请参阅警告和注意事项(5.1) ]
高血压[请参阅警告和注意事项(5.2) ]
心动过缓[请参阅警告和注意事项(5.3) ]
视觉障碍[请参阅警告和注意事项(5.4) ]
肌酸磷酸激酶(CPK)升高[请参阅警告和注意事项(5.5) ]
胰酶升高[见警告和注意事项(5.6) ]
高血糖[请参阅警告和注意事项(5.7) ]
6.1临床试验经验
由于临床试验是在广泛不同的条件下进行的,因此无法将在某种药物的临床试验中观察到的不良反应率直接与另一种药物的临床试验中观察到的不良反应率进行比较,并且可能无法反映实际中观察到的不良反应率。
在219名克唑替尼发生疾病进展后,在ALTA中接受了至少1剂ALUNBRIG的 219例局部晚期或转移性ALK阳性非小细胞肺癌(NSCLC)患者中,对ALUNBRIG的安全性进行了评估。患者连续90天每天一次接受ALUNBRIG 90毫克(90毫克组)或每天90毫克,连续7天,然后每天180毫克(90→180毫克组)。90 mg组的中位治疗时间为7.5个月,90→180 mg组的中位治疗时间为7.8个月。共有150(68%)名患者暴露于ALUNBRIG超过或等于6个月,而42(19%)名患者暴露于1年以上或等于1年。
研究人群的特征是:中位年龄54岁(范围:18至82岁),年龄小于65岁(77%),女性(57%),白人(67%),亚洲人(31%),第四阶段疾病( 98%),NSCLC腺癌组织学(97%),从不吸烟或曾经吸烟者(95%),ECOG表现状态(PS)0或1(93%)和基线时脑转移(69%)[参见临床研究(14 ) ]。
90 mg组中38%的患者和90→180 mg组中40%的患者发生了严重的不良反应。最常见的严重不良反应是肺炎(占整体的5.5%,在90 mg组为3.7%,在90→180 mg组中为7.3%)和ILD /肺炎(在整体上为4.6%,90 mg组为1.8%,占7.3) 90→180 mg组中的%)。致命不良反应发生在3.7%的患者中,包括肺炎(2例),猝死,呼吸困难,呼吸衰竭,肺栓塞,细菌性脑膜炎和尿道炎(各1例)。
在ALTA中,90 mg组的2.8%的患者和90→180 mg组的8.2%的患者因不良反应而永久停用ALUNBRIG。导致停药的最常见不良反应是ILD /肺炎(90 mg组为0.9%,90→180 mg组为1.8%)和肺炎(仅90→180 mg组为1.8%)。
在ALTA中,有14%的患者由于不良反应而需要降低剂量(90 mg组为7.3%,90→180 mg组为20%)。导致降低剂量的最常见不良反应是两种方案中的肌酸磷酸激酶升高(90 mg组为1.8%,90→180 mg组为4.5%)。
表3和表4总结了ALTA中常见的不良反应和实验室异常。
表3:按剂量组在ALTA(N = 219)中≥10%(所有等级*)或≥2%(3-4级)的患者的不良反应
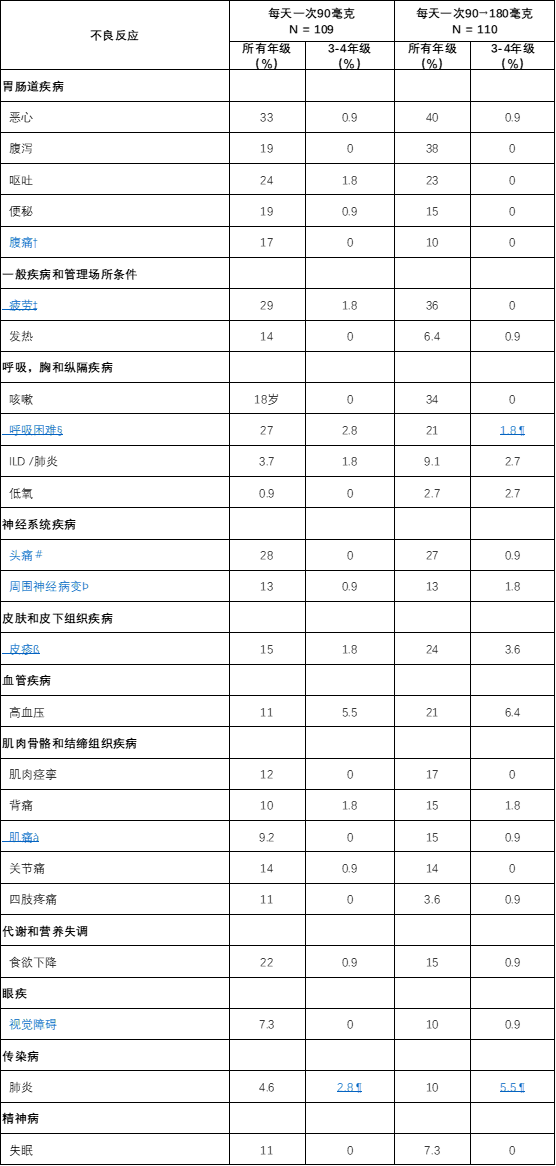
*根据国家癌症研究所不良事件通用术语标准(CTCAE)版本4.0
†包括腹胀,腹痛和上腹部不适
‡包括乏力和疲劳
§包括呼吸困难和劳累性呼吸困难
¶包括一项5年级活动
#包括头痛和窦性头痛
Þ包括周围感觉神经病和感觉异常
ß包括痤疮样皮炎,剥脱性皮疹,皮疹,瘙痒性皮疹和脓疱疹
一种包括肌肉骨骼疼痛和肌痛
è包括复视,畏光,视力模糊,视敏度降低,视力障碍,玻璃体漂浮物,视野缺损,黄斑水肿和玻璃体脱离
表4:ALTA中按方案的≥20%(所有等级*)患者的实验室异常(N = 219) 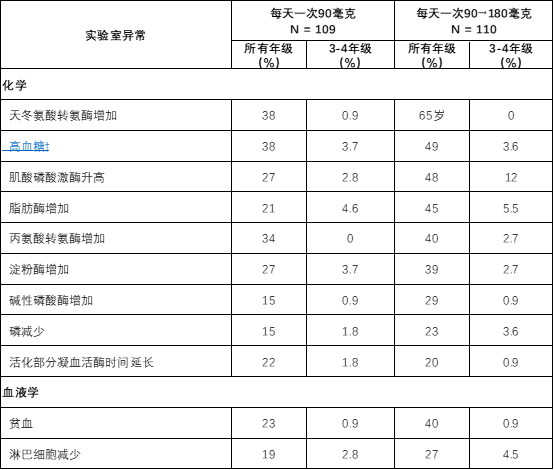
*根据CTCAE版本4.0
†两种方案中均观察到血液胰岛素升高
7药物相互作用
7.1其他药物对ALUNBRIG的影响
CYP3A抑制剂
将ALUNBRIG与强或中度CYP3A抑制剂共同给药会增加brigatinib血浆浓度,这可能会增加不良反应的发生率[见临床药理学(12.3) ]。避免将ALUNBRIG与强或中度CYP3A抑制剂并用。如果不能避免同时使用强效或中效CYP3A抑制剂,则按推荐的剂量调整剂量[见剂量和给药方法(2.3) ]。
强或中度CYP3A诱导剂
将ALUNBRIG与强或中度CYP3A诱导剂共同给药会降低brigatinib血浆浓度,这可能会降低ALUNBRIG 的疗效[见临床药理学(12.3) ]。避免将ALUNBRIG与强或中度CYP3A诱导剂共同给药。如果不能避免中度CYP3A诱导剂的共同给药,则根据建议调整剂量[见剂量和给药方法(2.4) ]。
7.2 ALUNBRIG对其他药物的影响
CYP3A底物
Brigatinib可能会降低CYP3A敏感底物的浓度。ALUNBRIG与CYP3A底物(包括激素避孕药)的共同给药可导致CYP3A敏感底物的浓度降低和功效丧失[见在特定人群中使用(8.3) ]。
8在特定人群中的使用
8.1怀孕
风险摘要
根据其作用机理和在动物中的发现,向孕妇服用ALUNBRIG可能会造成胎儿伤害[参见临床药理学(12.1) ]。没有关于孕妇使用ALUNBRIG的临床数据。在器官发生期间给怀孕的大鼠服用brigatinib会导致剂量相关的骨骼异常,剂量低至12.5 mg / kg /天(约为180毫克AUC每天一次的人暴露量的0.7倍),并且在术后增加或以25 mg / kg /天的剂量(约为人类每天180 mg暴露量的约1.26倍)植入或丢失,畸形和胎儿体重降低(参见数据)。建议孕妇注意胎儿的潜在危险。
在美国普通人群中,临床公认的怀孕中主要先天缺陷和流产的估计背景风险分别为2%至4%和15%至20%。
数据
动物资料
在一项胚胎-胎儿发育研究中,怀孕的大鼠在器官发生过程中每天服用brigatinib,观察到剂量相关的骨骼(骨化不完全,小门齿)和内脏异常,剂量低至12.5 mg / kg /天(约0.7)乘以每天一次180毫克AUC的人体暴露量)。以每天25 mg / kg /天(每天一次180 mg的人AUC的约1.26倍)观察到的畸形包括anasarca(全身性皮下水肿),失眼(无眼),前肢过度屈曲,小,短和/或弯曲的肢体,多次融合肋骨,弯曲的肩cap骨,卵圆形囊肿(肠突出到脐部)和胃痉挛(肠胃突出通过腹壁缺损),以及内脏发现侧脑室有中等程度的双侧扩张。
8.2哺乳
风险摘要
没有关于人乳中Brigatinib的分泌或其对母乳喂养婴儿或产奶量的影响的数据。由于母乳喂养婴儿可能产生不良反应,建议哺乳期妇女在ALUNBRIG治疗期间以及最终剂量后1周内不要母乳喂养。
8.3生殖潜力的男性和女性
验孕
在开始使用 ALUNBRIG 之前,请验证具有生殖潜能的女性的怀孕状况[请参阅在特定人群中使用(8.1) ]。
避孕
ALUNBRIG可能会造成胎儿伤害[请参阅在特定人群中使用(8.1) ]。
女性
建议有生殖潜力的女性在使用ALUNBRIG治疗期间以及最终剂量后至少4个月内使用有效的非激素避孕方法。建议患者使用非激素避孕方法,因为ALUNBRIG可以使某些激素避孕药无效[见药物相互作用(7.2) ]。
雄性
由于具有潜在的遗传毒性,建议具有生殖潜能的女性伴侣的男性在ALUNBRIG治疗期间以及最终剂量后至少3个月内使用有效的避孕方法[请参阅非临床毒理学(13.1) ]。
不孕症
根据动物雄性生殖器官的发现,ALUNBRIG可能导致雄性生育力降低[参见非临床毒理学(13.1) ]。
8.4小儿使用
尚未确定ALUNBRIG在儿科患者中的安全性和有效性。
8.5老年人使用
ALUNBRIG的临床研究未包括足够多的65岁及65岁以上的患者来确定他们对年轻患者的反应是否不同。
8.6肝功能不全
对于轻度肝功能不全(Child-Pugh A)或中度肝功能不全(Child-Pugh B)的患者,建议不调整剂量。减少重度肝功能不全(Child-Pugh C)患者的ALUNBRIG剂量[请参阅剂量和用法(2.5),临床药理学(12.3) ]。
8.7肾功能不全
对于轻度或中度肾功能不全的患者[Cockcroft-Gault肌酐清除率(CLcr)30至89 mL / min],建议不调整剂量。对于严重肾功能不全的患者(CLcr 15至29 mL / min),降低ALUNBRIG的剂量[参见剂量和用法(2.6),临床药理学(12.3) ]。
11说明
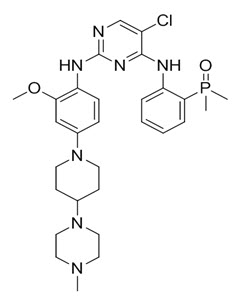
Brigatinib是一种激酶抑制剂。brigatinib的化学名称是5-氯-N 4- [2-(二甲基磷酰基)苯基] -N 2- {2-甲氧基-4- [4-(4-甲基哌嗪-1-基)哌啶-1-基]苯基}嘧啶-2,4-二胺。分子式为C 29 H 39 ClN 7 O 2 P,其分子式重量为584.10 g / mol。Brigatinib没有手性中心。化学结构如下所示:
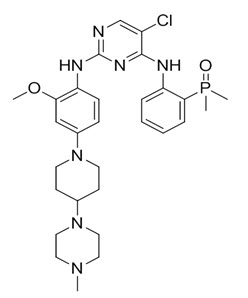
Brigatinib是灰白色至米色/棕褐色固体。的pK 一个被确定s至是:1.73±0.02(基峰),3.65±0.01(基峰),4.72±0.01(基极),和8.04±0.01(碱)。
ALUNBRIG以包含180 mg,90 mg或30 mg brigatinib和以下非活性成分的薄膜包衣片剂形式口服提供:乳糖一水合物,微晶纤维素,羟乙酸淀粉钠(A型),硬脂酸镁和疏水性胶 体二氧化硅。片剂包衣由滑石粉,聚乙二醇,聚乙烯醇和二氧化钛组成。
12临床药理学
12.1行动机制
Brigatinib是一种酪氨酸激酶抑制剂,在临床上可达到的浓度下对多种激酶具有体外活性,所述多种激酶包括ALK,ROS1,胰岛素样生长因子-1受体(IGF-1R)和FLT-3以及EGFR缺失和点突变。在体外和体内测定中, Brigatinib抑制ALK的自磷酸化和ALK介导的下游信号蛋白STAT3,AKT,ERK1 / 2和S6的磷酸化。Brigatinib还抑制表达EML4-ALK和NPM-ALK融合蛋白的细胞系的体外增殖,并证明剂量依赖性抑制小鼠EML4-ALK阳性NSCLC异种移植的生长。
在临床可达到的浓度(≤500nM)下,Brigatinib抑制表达EML4-ALK和17种与ALK抑制剂(包括克唑替尼)和EGFR-Del(E746-A750),ROS1-L2026M的耐药性相关的突变形式的细胞的体外存活力,FLT3-F691L和FLT3-D835Y。Brigatinib 对EML4-ALK的4种突变体表现出体内抗肿瘤活性,包括在克唑替尼治疗的患者中在NSCLC肿瘤中鉴定出的G1202R和L1196M突变体。Brigatinib还可减轻颅骨内植入ALK驱动的肿瘤细胞系的小鼠的肿瘤负担并延长其生存期。
12.2药效学
Brigatinib暴露-反应关系和药效学反应的时间过程是未知的。
心脏电生理学
在每天一次ALUNBRIG剂量为30毫克(180毫克推荐剂量的0.16倍)至240毫克(180毫克推荐剂量的1.3倍)之后,对123名患者评估了ALUNBRIG的QT间隔延长潜力。ALUNBRIG并未将QT间隔延长至临床相关程度。
12.3药代动力学
的几何平均值(CV%)稳态最大浓度(C 最大值 brigatinib的)在ALUNBRIG剂量90毫克和180毫克,每天一次为552(65%)ng / mL和1452(60%)纳克/毫升,分别浓度-时间曲线下的相应面积(AUC 0-Tau)为8165(57%)ng∙h / mL和20276(56%)ng∙h / mL。在单剂量和多次给药ALUNBRIG之后,每天一次的brigatinib全身暴露剂量范围为60 mg(180毫克推荐剂量的0.3倍)至240 mg(180毫克推荐剂量的1.3倍)。重复给药后的平均积累比为1.9至2.4。
吸收性
在单次口服ALUNBRIG剂量为30 mg至240 mg之后,达到峰值浓度的中位时间(T max)为1-4小时。
食物的作用
与过夜禁食后的C max和AUC 相比,高脂餐后(约920卡路里,58克碳水化合物,59克脂肪和40克蛋白质)服用ALUNBRIG的健康受试者的Brigatinib C max降低了13%,对AUC无影响。
分配
Brigatinib与人血浆蛋白结合的比例为91%,并且该结合不是浓度依赖性的。血液与血浆的浓度比为0.69。每天一次口服ALUNBRIG 180 mg后,稳定状态下brigatinib 的平均表观分布体积(V z / F)为153L。
消除
每天一次口服ALUNBRIG 180 mg后,稳定状态下brigatinib的平均表观口服清除率(CL / F)为12.7 L / h,平均血浆清除半衰期为25小时。
代谢
Brigatinib 在体外主要通过CYP2C8和CYP3A4代谢。在向健康受试者口服单次180 mg剂量的放射性标记的brigatinib之后,N-去甲基化和半胱氨酸结合是两个主要的代谢途径。不变的brigatinib(92%)是主要的循环放射性成分。
排泄
向健康受试者口服单次180 mg剂量的放射性标记的brigatinib后,粪便中回收了65%的剂量,尿液中回收了25%的剂量。不变的brigatinib分别占粪便和尿液总放射性的41%和86%。
特定人群
年龄,种族,性别,体重和白蛋白浓度对Brigatinib的药代动力学没有临床意义的影响。
肝功能不全患者
服用单剂量ALUNBRIG 90 mg后,严重肝功能不全(Child-Pugh C)患者的未结合brigatinib全身暴露(AUC 0-INF)比正常肝功能患者高37%。轻度(Child-Pugh A)到中度(Child-Pugh B)肝功能不全的受试者与肝功能正常的受试者之间的未结合Brigatinib全身暴露(AUC 0-INF)相似[参见剂量和给药方法(2.5) ]。
肾功能不全的患者
服用单剂ALUNBRIG 90 mg后,严重肾功能不全[肌酐清除率(CLcr)15至29 mL / min]的患者与正常肾功能的患者相比,未结合的brigatinib全身暴露(AUC 0-INF)高86%。
根据人群药代动力学分析,在125例轻度肾功能不全(CLcr 60至89 mL / min),34例中度肾功能不佳(CLcr 30至59 mL / min)和270例肾功能正常的受试者中,Brigatinib的暴露情况相似(CLcr≥90mL / min)[参见剂量和用法(2.6) ]。
药物相互作用研究
临床研究
CYP3A强抑制剂对Brigatinib的作用:
与单个90毫克的剂量的200 mg,每天两次的剂量依他康唑的(较强的CYP3A抑制剂)共同给药ALUNBRIG增加brigatinibÇ 最大 21%和AUC 0-INF 101%,相对于90毫克的剂量的ALUNBRIG单独给药[参见剂量和用法(2.3),药物相互作用(7.1) ]。预计中度CYP3A抑制剂会使brigatinib的AUC升高约40%。
强效CYP2C8抑制剂对Brigatinib的影响:
与单个90毫克的剂量的600 mg,每天两次剂量吉非贝齐的(较强的CYP2C8抑制剂)共同给药ALUNBRIG降低brigatinibÇ 最大 41%和AUC 0-INF 12%,相对于90毫克的剂量的ALUNBRIG单独给药。吉非贝齐对brigatinib药代动力学的影响在临床上没有意义,并且降低brigatinib暴露的潜在机制尚不清楚。
强和中度CYP3A诱导剂对Brigatinib的影响:
与单一180毫克剂量的600毫克的日剂量利福平(一个强CYP3A诱导剂)联合给药ALUNBRIG降低brigatinibÇ 最大 60%和AUC 0-INF至180毫克的剂量的80%,相对于ALUNBRIG单独给药[见剂量和用法(2.4),药物相互作用(7.1) ]。预计中度CYP3A诱导剂会使brigatinib的AUC降低约50%。
体外研究
Brigatinib对CYP酶的影响:
Brigatinib在临床上相关的血浆浓度下,通过激活孕烷X受体(PXR)诱导CYP3A。Brigatinib也可能通过相同的机制在临床相关浓度下诱导CYP2C酶。
在临床相关浓度下,Brigatinib不会抑制CYP1A2、2B6、2C8、2C9、2C19、2D6或3A4 / 5。
P-糖蛋白和BCRP抑制剂对Brigatinib的影响:
Brigatinib是外排转运蛋白P-糖蛋白(P-gp)和乳腺癌抗性蛋白(BCRP)的底物。鉴于brigatinib 在体外具有高溶解度和高渗透性,因此P-gp和BCRP抑制剂不太可能增加brigatinib的血浆浓度。
其他转运蛋白对Brigatinib的影响:
Brigatinib不是有机阴离子转运多肽(OATP1B1,OATP1B3),有机阴离子转运蛋白(OAT1,OAT3),有机阳离子转运蛋白(OCT1,OCT2),多药和毒素挤出蛋白(MATE1,MATE2K)或胆盐输出泵的底物(BSEP)。
Brigatinib对转运蛋白的影响:
Brigatinib是P-gp,BCRP,OCT1,MATE1和MATE2K 的体外抑制剂。因此,Brigatinib可能具有增加这些转运蛋白共同施用底物浓度的潜力。临床相关浓度的Brigatinib不会抑制OATP1B1,OATP1B3,OAT1,OAT3,OCT2或BSEP。
13毒理学
13.1致癌,诱变,生育力受损
Brigatinib尚未进行致癌性研究。
用brigatinib治疗会导致大鼠体内哺乳动物红细胞微核中的染色体损伤,但在Ames或体外哺乳动物染色体畸变测试中没有致突变性。
没有使用brigatinib进行专门的动物生育力研究。在重复剂量的动物研究中,观察到的睾丸毒性导致其暴露量低至180毫克患者暴露量的0.2倍。在大鼠中,发现的疾病包括睾丸,精囊和前列腺的重量降低,以及睾丸小管变性。这些效果在2个月的恢复期内不可逆。在猴子中,发现的结果包括睾丸尺寸减小以及镜下发生精子发生的证据。在恢复期间,这些影响是可逆的。
14临床研究
ALUNBRIG的功效在一项两臂,开放标签,多中心试验(ALTA,NCT02094573)中证实,对于已接受克唑替尼治疗的局部晚期或转移性ALK阳性非小细胞肺癌(NSCLC)成年患者。该研究的患者需要根据FDA批准的试验或不同的测试由Vysis公司足够的存档组织确认ALK安排有书面ALK重排®ALK Break-Apart荧光原位杂交(FISH)探针试剂盒测试。关键资格标准包括ECOG绩效状态为0-2和克唑替尼治疗进展。具有中枢神经系统(CNS)转移的神经学稳定的患者被允许参加。排除有间质性肺病或药物相关性肺炎病史或在首次服用布列加替尼3天内接受克唑替尼治疗的患者。根据独立审查委员会(IRC)评估的实体瘤反应评估标准(RECIST v1.1),确认主要疗效结局指标为总体反应率(ORR)。其他功效结果指标包括研究者评估的ORR,反应持续时间(DOR),颅内ORR和颅内DOR。
总共222例患者被随机分配接受ALUNBRIG每天90 mg(每天90 mg; n = 112);每天7次口服90 mg(每天90mg→180 mg;每天手臂90 mg; n = 112);每天一次180 mg。 = 110)。根据脑转移(存在或不存在)和对克唑替尼的最佳先前反应(完全或部分反应与任何其他反应/无法评估)进行分层。
总体研究人群的基线人口统计学特征是:中位年龄54岁(年龄在18至82岁之间,年龄在65%以上的人群为23%),白人为67%,亚洲为31%,女性为57%,ECOG PS 0为57%,ECOG PS 1为57 ,还有95%从不吸烟或曾经吸烟的人。总体研究人群的疾病特征为:IV期疾病占98%,腺癌组织学占97%,先前的全身化学疗法占74%,脑转移性疾病占69%(61%曾接受过脑部放射治疗), 39%的患者发生骨转移,26%的患者发生肝转移。64%的患者对既往的克唑替尼有客观反应。
中位随访时间为8个月(范围:0.1-20.2)。表5总结了ALTA的疗效结果。
表5:ALTA功效结果
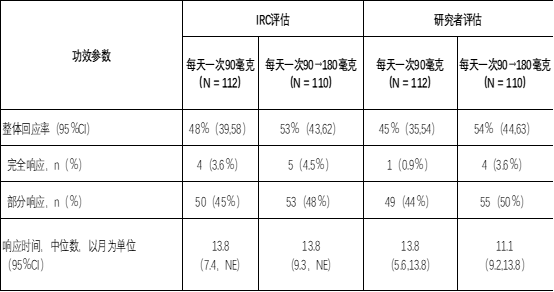
CI =置信区间;NE =不可估计
表6总结了根据RECIST v1.1对基线时可测量的脑转移(最长直径≥10mm)的44例亚组患者进行的颅内ORR和颅内DOR的IRC评估。表6总结了颅内反应的持续时间颅内反应直至颅内疾病进展(新病变,颅底目标病变直径从最低点增长≥20%或颅内非目标病变明确进展)或死亡。
表6:ALTA中可测量的脑转移患者的颅内总体反应
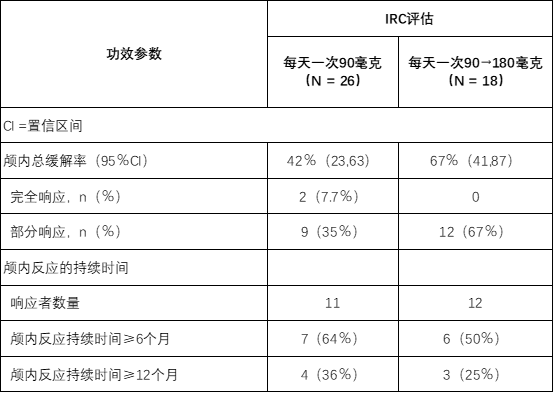
CI =置信区间
16供应/存储和处理方式
180 mg片剂:椭圆形,白色至类白色薄膜衣片,一侧凹陷有“ U13”,另一侧凹陷。可用于:

90 mg片剂:椭圆形,白色至类白色薄膜衣片,一侧凹陷有“ U7”,另一侧凹陷。可用于:

30 mg片剂:圆形,白色至类白色薄膜衣片,一侧凹陷有“ U3”,另一侧为平纹;可用于:

90毫克/ 7粒片剂(NDC 63020-090-07)和180毫克/ 23粒片剂(NDC 63020-180-23)也可以在一个纸箱中作为一个月的初始包装使用:
存放在20°C至25°C(68°F至77°F)的受控室温下; 在15°C至30°C(59°F至86°F)之间允许的偏移(请参阅USP)。
17患者咨询信息
建议患者阅读FDA批准的患者标签(患者信息)。
间质性肺疾病(ILD)/肺炎
告知患者严重的肺部不良反应(如ILD /肺炎)的症状和风险。劝告患者立即报告任何新的或恶化的呼吸道症状[见警告和注意事项(5.1) ]。
高血压
告知有高血压危险的患者,并及时报告高血压的体征或症状[见警告和注意事项(5.2) ]。
心动过缓
劝告患者报告心动过缓的任何症状,并告知其医疗保健人员有关使用心脏和血压药物的信息[请参阅警告和注意事项(5.3) ]。
视觉障碍
建议患者将任何新的或恶化的视力症状告知其医疗保健提供者[请参阅警告和注意事项(5.4) ]。
肌酸磷酸激酶(CPK)升高
告知患者肌酸酐磷酸激酶(CPK)升高的体征和症状以及治疗期间需要进行监测。建议患者将无法解释的肌肉疼痛,压痛或无力的任何新的或恶化的症状告知其医疗保健提供者[请参阅警告和注意事项(5.5) ]。
胰酶升高
告知患者胰腺炎的体征和症状,以及在治疗期间需要监测淀粉酶和脂肪酶的升高[见警告和注意事项(5.6) ]。
高血糖症
告知患者出现新的或恶化的高血糖症的风险,以及需要定期监测血糖水平的情况。告知患有糖尿病或葡萄糖耐量异常的患者,在使用ALUNBRIG 治疗期间可能需要调整抗高血糖药物[见警告和注意事项(5.7) ]。
生殖潜力的男性和女性
胚胎-胎儿毒性
告知具有生殖潜力的雌性和雄性,ALUNBRIG可能会造成胎儿伤害[请参阅警告和注意事项(5.8),在特定人群中使用(8.1) ]。
建议有生殖能力的女性告知其保健服务提供者已知或疑似怀孕,并在使用ALUNBRIG治疗期间以及最终剂量后至少4个月内使用有效的非激素避孕药(请参见“ 在特定人群中使用(8.3) ”)。
建议具有生殖潜能的女性伴侣的男性在ALUNBRIG治疗期间以及最终剂量后至少3个月内使用有效的避孕药[请参见在特定人群中使用(8.3) ]。
哺乳期
劝告女性在使用ALUNBRIG治疗期间以及最终剂量后至少1周内不要母乳喂养[参见在特定人群中使用(8.2) ]。
不孕症
劝告男性从ALUNBRIG 降低生育能力的生殖潜力[请参见“ 在特殊人群中使用(8.3),非临床毒理学(13.1) ”。
药物相互作用
建议患者将所有伴随药物(包括处方药,非处方药,维生素和草药产品)告知其医疗保健提供者。告知患者在服用ALUNBRIG时 避免服用葡萄柚或葡萄柚汁[见药物相互作用(7) ]。
剂量和给药
指导患者在前7天每天服用90毫克ALUNBRIG,如果可以忍受的话,将剂量增加到每天180毫克。建议患者在有或没有食物的情况下服用ALUNBRIG [见剂量和用法(2.1) ]。
错过剂量
告知患者,如果错过了ALUNBRIG剂量,或者如果患者在服用ALUNBRIG剂量后呕吐,则不要在常规时间服用额外剂量,而应再服用下一剂[见剂量和用法(2.1) ]。
制造用于:
武田制药有限公司
马萨诸塞州剑桥,40 Landsdowne Street,02139-4234
ALUNBRIG ®是ARIAD制药公司武田药品有限公司的全资子公司的注册商标。
©2017-2018 ARIAD Pharmaceuticals,Inc.保留所有权利。
ABG346 R2
患者信息
ALUNBRIG(uh-lun-brig)
(brigatinib)
片剂患者信息
ALUNBRIG(uh-lun-brig)
(brigatinib)
片剂我应该了解的有关ALUNBRIG的最重要信息是什么?
ALUNBRIG可能会导致严重的副作用,包括:肺部问题。在治疗期间,ALUNBRIG可能会导致严重的或危及生命的肺部肿胀(发炎),并可能导致死亡。这些肺部疾病尤其在使用ALUNBRIG 治疗的第一周内发生。症状可能与肺癌的症状相似。如果您有任何新的或恶化的症状,请立即告诉您的医疗保健提供者,包括:
呼吸困难或呼吸急促
胸痛
有或没有粘液的咳嗽
发热
高血压(高血压)。 ALUNBRIG可能会导致高血压。您的医疗保健提供者将在开始使用ALUNBRIG之前和进行治疗期间检查您的血压。如果您出现头痛,头晕,视力模糊,胸痛或呼吸急促,请立即告知您的医疗服务提供者。
心律缓慢(心动过缓)。 ALUNBRIG可能会导致非常缓慢的心跳,可能非常严重。您的医疗保健提供者将在使用ALUNBRIG治疗期间检查您的心律。如果您在使用ALUNBRIG治疗期间感到头晕,头晕或晕眩,请立即告诉您的医疗服务提供者。告诉您的医疗保健提供者您是否开始服用或改变心脏或血压药物。
视力问题。 ALUNBRIG可能会导致视力问题。如果您在使用ALUNBRIG进行治疗时出现严重的视力问题,您的医疗保健提供者可能会停止ALUNBRIG并转介给眼科医生。如果您有视力丧失或视力变化,请立即告知您的医疗保健提供者,包括:
双重视野
看到闪光灯
视力模糊
轻伤眼睛
新的或增加的流动人口
肌肉疼痛,压痛和无力(肌痛)。 ALUNBRIG可能会增加血液中一种称为肌酸磷酸激酶(CPK)的酶的水平,这可能是肌肉损伤的迹象。您的医疗保健提供者将在ALUNBRIG治疗期间进行血液检查,以检查您的CPK血液水平。如果您发现新的或恶化的肌肉问题迹象和症状,包括无法解释的肌肉疼痛或无法消失的肌肉疼痛,压痛或无力,请立即告知您的医疗服务提供者。
胰腺发炎(胰腺炎)。 ALUNBRIG可能会增加血液中的淀粉酶和脂肪酶,这可能是胰腺炎的征兆。在使用ALUNBRIG治疗期间,您的医疗保健提供者将进行血液检查以检查您的胰酶血液水平。如果您出现新的或恶化的胰腺炎体征和症状,包括上腹部疼痛,可能会蔓延到背部,并因进食,体重减轻或恶心而恶化,请立即告知您的医护人员。
高血糖(高血糖症)。 ALUNBRIG可能会增加您的血糖水平。您的医疗保健提供者将在开始使用ALUNBRIG之前和治疗期间进行血液检查,以检查您的血糖水平。您的医疗保健提供者可能需要开始或更改血糖药物以控制血糖水平。如果您发现新的或恶化的高血糖症状和体征,请立即告知您的医疗保健提供者,包括:
感到很口渴
需要比平时更多的小便
感觉很饿
肚子不舒服
感到虚弱或疲倦
感觉困惑
有关副作用的信息,请参见“ ALUNBRIG的可能副作用是什么? ” 什么是ALUNBRIG?
ALUNBRIG是用于治疗非小细胞肺癌(NSCLC)的处方药:具有某种类型的异常性间变性淋巴瘤激酶(ALK)基因,并且
已经扩散到您身体的其他部位,并且
服用克唑替尼但他们的非小细胞肺癌恶化或他们不能忍受克唑替尼的人。
尚不知道ALUNBRIG在儿童中是否安全有效。
服用ALUNBRIG之前,请告知您的医疗保健提供者所有您的医疗状况,包括是否:
有肺或呼吸问题
有高血压
心跳慢
有视力问题
患有或曾经患有胰腺炎
患有糖尿病或葡萄糖耐量
有肝脏问题
有肾脏问题或正在透析
正在怀孕或打算怀孕。ALUNBRIG可能会伤害未出生的婴儿。在开始使用ALUNBRIG治疗之前,您的医疗保健提供者将确定您是否怀孕。如果您在使用ALUNBRIG治疗期间怀孕或认为自己可能怀孕,请立即告诉您的医疗保健提供者。
能够怀孕的女性在ALUNBRIG治疗期间以及ALUNBRIG最终剂量后至少4个月内应使用有效的非激素避孕措施。如果在ALUNBRIG治疗期间使用避孕药(口服避孕药)和其他激素控制型避孕药可能无效。与您的医疗保健提供者谈谈使用ALUNBRIG治疗期间适合您的节育选择。
具有女性伴侣能够怀孕的男性应该在ALUNBRIG治疗期间和最终剂量ALUNBRIG给药后至少3个月内使用有效的避孕方法。
正在母乳喂养或计划母乳喂养。尚不知道ALUNBRIG是否会进入母乳。在用ALUNBRIG治疗期间和最终剂量ALUNBRIG用药后1周内不要母乳喂养。
告诉您的医疗保健提供者您服用的所有药物,包括处方药,非处方药,维生素或草药补品。
我应该如何服用ALUNBRIG?
完全按照医护人员的指示服用ALUNBRIG。除非您的医疗保健提供者告诉您,否则请勿更改剂量或停止服用ALUNBRIG。
您的医疗保健提供者将在治疗的前7天以低剂量(90 mg)的ALUNBRIG开始治疗。如果您能够很好地耐受此剂量的ALUNBRIG,则您的医疗保健提供者可能会在治疗的前7天增加您的剂量。
如果您出现副作用,您的医疗服务提供者可能会更改您的剂量,暂时停止或永久停止使用ALUNBRIG的治疗。
就拿ALUNBRIG 1次的每一天。
带或不带食物一起服用ALUNBRIG。
吞下整个ALUNBRIG片剂。不要压碎或咀嚼药片。
如果您错过了ALUNBRIG剂量,请勿服用错过的剂量。在正常时间服用下一次剂量。
如果您在服用ALUNBRIG后呕吐,请勿再服用。在正常时间服用下一次剂量。
服用ALUNBRIG时应该避免什么?
在使用ALUNBRIG进行治疗时,避免吃西柚或喝西柚汁。葡萄柚可能会增加血液中ALUNBRIG的含量。
ALUNBRIG可能有哪些副作用?
ALUNBRIG可能会导致严重的副作用,包括:请参阅“ 关于ALUNBRIG我应该了解的最重要的信息是什么? ”
ALUNBRIG最常见的副作用包括:
恶心
腹泻
疲劳
咳嗽
头痛 ALUNBRIG可能导致男性生育问题。这可能会影响您生孩子的能力。如果您担心生育,请与您的医疗保健提供者联系。
这些并非ALUNBRIG的所有可能的副作用。
打电话给您的医生,征求有关副作用的医疗建议。您可以通过1-800-FDA-1088向FDA报告副作用。我应该如何存储ALUNBRIG?
将ALUNBRIG存放在20°C至25°C(68°F至77°F)的室温下。
将ALUNBRIG和所有药品放在儿童接触不到的地方。
有关安全有效使用ALUNBRIG的一般信息。
有时出于患者信息手册中列出的目的以外的目的开出处方药。请勿在未指定条件的情况下使用ALUNBRIG。即使他人有相同的症状,也请勿将ALUNBRIG给予他人。可能会伤害他们。
您可以询问您的医疗保健提供者或药剂师以获取有关ALUNBRIG的信息,这些信息是为卫生专业人员编写的。ALUNBRIG中的成分是什么?
活性成分: brigatinib惰性
成分:乳糖一水合物,微晶纤维素,羟乙酸淀粉钠(A型),硬脂酸镁和疏水性胶体二氧化硅。片剂包衣由滑石粉,聚乙二醇,聚乙烯醇和二氧化钛组成。
生产厂商:武田制药有限公司,马萨诸塞州剑桥市兰茨敦街40号,马萨诸塞州02139-4234。ALUNBRIG ®是ARIAD制药公司武田药品有限公司的全资子公司的注册商标。©2017-2018 ARIAD Pharmaceuticals,Inc.保留所有权利。
有关更多信息,请访问www。阿伦布里格.com或致电1-844-A-1POINT(1-844-217-6468)。该患者信息已获得美国食品和药物管理局的批准 ABG346 R2 修订日期:2018年12月 主要显示面板-30毫克片剂瓶纸箱
NDC 63020-113-30
ALUNBRIG ™
(brigatinib)片剂30毫克
仅接收
30片
主要显示面板-90毫克片剂瓶纸箱
NDC 63020-090-30
ALUNBRIG ™
(brigatinib)片剂90毫克
仅接收
30片
主要显示面板-180毫克片剂瓶纸箱
NDC 63020-180-30
ALUNBRIG ™
(brigatinib)片剂180毫克
仅接收
30片
主要显示面板-套件纸箱
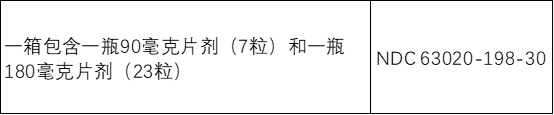
NDC 63020-198-30初始化
包ALUNBRIG ™
(brigatinib)片剂仅接收| 口服使用
常规剂量:前7天每天口服一次90毫克片剂;
如果可以忍受,则每天口服一次,增加至180 mg片剂。
有关完整的详细信息,请参见随附的完整“处方信息”。90毫克
7片
第1天-第7天服用1片180毫克
23片
第8天-第30天服用1片
-
本说明书来源于:美国FDA
https://nctr-crs.fda.gov/fdalabel/services/spl/set-ids/0fe9ff20-d402-41f3-bc1e-7002ea7007db/spl-doc?hl=ALUNBRIG
温馨提醒:
①建议您用 谷歌浏览器 在电脑上或手机 打开以上链接,就可以自动翻译成简体中文,而且翻译的还比较准确。
②本说明书仅供参考,最新的说明书详见药品附带的说明书
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
ALUNBRIG is indicated for the treatment of patients with anaplastic lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) who have progressed on or are intolerant to crizotinib.
This indication is approved under accelerated approval based on tumor response rate and duration of response [see Clinical Studies (14)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial.
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
The recommended dosage for ALUNBRIG is:
90 mg orally once daily for the first 7 days;
if 90 mg is tolerated during the first 7 days, increase the dose to 180 mg orally once daily.
Administer ALUNBRIG until disease progression or unacceptable toxicity.
If ALUNBRIG is interrupted for 14 days or longer for reasons other than adverse reactions, resume treatment at 90 mg once daily for 7 days before increasing to the previously tolerated dose.
ALUNBRIG may be taken with or without food. Instruct patients to swallow tablets whole. Do not crush or chew tablets.
If a dose of ALUNBRIG is missed or vomiting occurs after taking a dose, do not administer an additional dose and take the next dose of ALUNBRIG at the scheduled time.
2.2 Dosage Modifications for Adverse Reactions
ALUNBRIG dosage reductions for adverse reactions are summarized in Table 1.
Table 1: Recommended ALUNBRIG Dosage Reductions

*Not applicable
Once reduced for adverse reactions, do not subsequently increase the dosage of ALUNBRIG. Permanently discontinue ALUNBRIG if patients are unable to tolerate the 60 mg once daily dose.
Recommendations for dosage modifications of ALUNBRIG for the management of adverse reactions are provided in Table 2.
Table 2: Recommended ALUNBRIG Dosage Modifications for Adverse Reactions
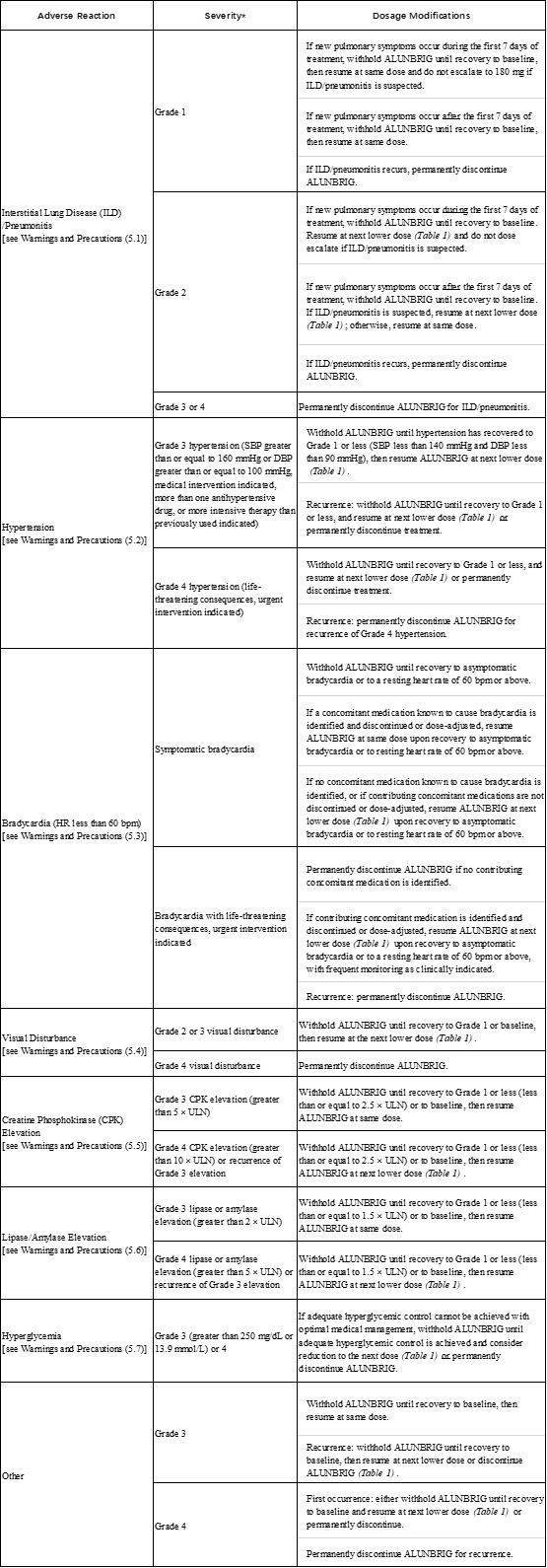
bpm = beats per minute; DBP = diastolic blood pressure; HR = heart rate; SBP = systolic blood pressure; ULN = upper limit of normal
*Graded per National Cancer Institute Common Terminology Criteria for Adverse Events. Version 4.0 (NCI CTCAE v4).
2.3 Dosage Modifications for Strong or Moderate CYP3A Inhibitors
Avoid coadministration of strong or moderate CYP3A inhibitors during treatment with ALUNBRIG [see Drug Interactions (7.1), Clinical Pharmacology (12.3)]. If coadministration of a strong CYP3A inhibitor cannot be avoided, reduce the ALUNBRIG once daily dose by approximately 50% (i.e. from 180 mg to 90 mg, or from 90 mg to 60 mg). If coadministration of a moderate CYP3A inhibitor cannot be avoided, reduce the ALUNBRIG once daily dose by approximately 40% (i.e. from 180 mg to 120 mg, 120 mg to 90 mg, or from 90 mg to 60 mg). After discontinuation of a strong or moderate CYP3A inhibitor, resume the ALUNBRIG dose that was tolerated prior to initiating the CYP3A inhibitor.
2.4 Dosage Modifications for Moderate CYP3A Inducers
Avoid coadministration of moderate CYP3A inducers during treatment with ALUNBRIG [see Drug Interactions (7.1), Clinical Pharmacology (12.3)]. If coadministration of a moderate CYP3A inducer cannot be avoided, increase the ALUNBRIG once daily dose in 30 mg increments after 7 days of treatment with the current ALUNBRIG dose as tolerated, up to a maximum of twice the ALUNBRIG dose that was tolerated prior to initiating the moderate CYP3A inducer.
After discontinuation of a moderate CYP3A inducer, resume the ALUNBRIG dose that was tolerated prior to initiating the moderate CYP3A inducer.
2.5 Dosage Modifications for Patients with Severe Hepatic Impairment
Reduce the ALUNBRIG once daily dose by approximately 40% (i.e. from 180 mg to 120 mg, 120 mg to 90 mg, or from 90 mg to 60 mg) for patients with severe hepatic impairment (Child-Pugh C) [see Use in Specific Populations (8.6), Clinical Pharmacology (12.3)].
2.6 Dosage Modifications for Patients with Severe Renal lmpairment
Reduce the ALUNBRIG once daily dose by approximately 50% (i.e. from 180 mg to 90 mg, or from 90 mg to 60 mg) for patients with severe renal impairment [creatinine clearance (CLcr) 15 to 29 mL/min by Cockcroft-Gault] [see Use in Specific Populations (8.7), Clinical Pharmacology (12.3)].
3 DOSAGE FORMS AND STRENGTHS
180 mg: oval, white to off-white film-coated tablets with "U13" debossed on one side and plain on the other side
90 mg: oval, white to off-white film-coated tablets with "U7" debossed on one side and plain on the other side
30 mg: round, white to off-white film-coated tablets with "U3" debossed on one side and plain on the other side
4 CONTRAINDICATIONS
None.
5 WARNINGS AND PRECAUTIONS
5.1 Interstitial Lung Disease (ILD)/Pneumonitis
Severe, life-threatening, and fatal pulmonary adverse reactions consistent with interstitial lung disease (ILD)/pneumonitis have occurred with ALUNBRIG.
In Trial ALTA (ALTA), ILD/pneumonitis occurred in 3.7% of patients in the 90 mg group (90 mg once daily) and 9.1% of patients in the 90→180 mg group (180 mg once daily with 7-day lead-in at 90 mg once daily).
Adverse reactions consistent with possible ILD/pneumonitis occurred early (within 9 days of initiation of ALUNBRIG; median onset was 2 days) in 6.4% of patients, with Grade 3 to 4 reactions occurring in 2.7%.
Monitor for new or worsening respiratory symptoms (e.g., dyspnea, cough, etc.), particularly during the first week of initiating ALUNBRIG. Withhold ALUNBRIG in any patient with new or worsening respiratory symptoms, and promptly evaluate for ILD/pneumonitis or other causes of respiratory symptoms (e.g., pulmonary embolism, tumor progression, and infectious pneumonia). For Grade 1 or 2 ILD/pneumonitis, either resume ALUNBRIG with dose reduction according to Table 1 after recovery to baseline or permanently discontinue ALUNBRIG. Permanently discontinue ALUNBRIG for Grade 3 or 4 ILD/pneumonitis or recurrence of Grade 1 or 2 ILD/pneumonitis [see Dosage and Administration (2.2), Adverse Reactions (6.1)].
5.2 Hypertension
In ALTA, hypertension was reported in 11% of patients in the 90 mg group who received ALUNBRIG and 21% of patients in the 90→180 mg group. Grade 3 hypertension occurred in 5.9% of patients overall.
Control blood pressure prior to treatment with ALUNBRIG. Monitor blood pressure after 2 weeks and at least monthly thereafter during treatment with ALUNBRIG. Withhold ALUNBRIG for Grade 3 hypertension despite optimal antihypertensive therapy. Upon resolution or improvement to Grade 1 severity, resume ALUNBRIG at a reduced dose. Consider permanent discontinuation of treatment with ALUNBRIG for Grade 4 hypertension or recurrence of Grade 3 hypertension [see Dosage and Administration (2.2), Adverse Reactions (6.1)].
Use caution when administering ALUNBRIG in combination with antihypertensive agents that cause bradycardia [see Warnings and Precautions (5.3)].
5.3 Bradycardia
Bradycardia can occur with ALUNBRIG. In ALTA, heart rates less than 50 beats per minute (bpm) occurred in 5.7% of patients in the 90 mg group and 7.6% of patients in the 90→180 mg group. Grade 2 bradycardia occurred in 1 (0.9%) patient in the 90 mg group.
Monitor heart rate and blood pressure during treatment with ALUNBRIG. Monitor patients more frequently if concomitant use of drug known to cause bradycardia cannot be avoided [see Warnings and Precautions (5.2)].
For symptomatic bradycardia, withhold ALUNBRIG and review concomitant medications for those known to cause bradycardia. If a concomitant medication known to cause bradycardia is identified and discontinued or dose adjusted, resume ALUNBRIG at the same dose following resolution of symptomatic bradycardia; otherwise, reduce the dose of ALUNBRIG following resolution of symptomatic bradycardia. Discontinue ALUNBRIG for life-threatening bradycardia if no contributing concomitant medication is identified [see Dosage and Administration (2.2)].
5.4 Visual Disturbance
In ALTA, adverse reactions leading to visual disturbance including blurred vision, diplopia, and reduced visual acuity, were reported in 7.3% of patients receiving ALUNBRIG in the 90 mg group and 10% of patients in the 90→180 mg group. Grade 3 macular edema and cataract occurred in 1 patient each in the 90→180 mg group.
Advise patients to report any visual symptoms. Withhold ALUNBRIG and obtain an ophthalmologic evaluation in patients with new or worsening visual symptoms of Grade 2 or greater severity. Upon recovery of Grade 2 or Grade 3 visual disturbances to Grade 1 severity or baseline, resume ALUNBRIG at a reduced dose. Permanently discontinue treatment with ALUNBRIG for Grade 4 visual disturbances [see Dosage and Administration (2.2), Adverse Reactions (6.1)].
5.5 Creatine Phosphokinase (CPK) Elevation
In ALTA, creatine phosphokinase (CPK) elevation occurred in 27% of patients receiving ALUNBRIG in the 90 mg group and 48% of patients in the 90 mg→180 mg group. The incidence of Grade 3-4 CPK elevation was 2.8% in the 90 mg group and 12% in the 90→180 mg group.
Dose reduction for CPK elevation occurred in 1.8% of patients in the 90 mg group and 4.5% in the 90→180 mg group.
Advise patients to report any unexplained muscle pain, tenderness, or weakness. Monitor CPK levels during ALUNBRIG treatment. Withhold ALUNBRIG for Grade 3 or 4 CPK elevation. Upon resolution or recovery to Grade 1 or baseline, resume ALUNBRIG at the same dose or at a reduced dose as described in Table 2 [see Dosage and Administration (2.2), Adverse Reactions (6.1)].
5.6 Pancreatic Enzymes Elevation
In ALTA, amylase elevation occurred in 27% of patients in the 90 mg group and 39% of patients in the 90→180 mg group. Lipase elevations occurred in 21% of patients in the 90 mg group and 45% of patients in the 90→180 mg group. Grade 3 or 4 amylase elevation occurred in 3.7% of patients in the 90 mg group and 2.7% of patients in the 90→180 mg group. Grade 3 or 4 lipase elevation occurred in 4.6% of patients in the 90 mg group and 5.5% of patients in the 90→180 mg group.
Monitor lipase and amylase during treatment with ALUNBRIG. Withhold ALUNBRIG for Grade 3 or 4 pancreatic enzyme elevation. Upon resolution or recovery to Grade 1 or baseline, resume ALUNBRIG at the same dose or at a reduced dose as described in Table 2 [see Dosage and Administration (2.2), Adverse Reactions (6.1)].
5.7 Hyperglycemia
In ALTA, 43% of patients who received ALUNBRIG experienced new or worsening hyperglycemia. Grade 3 hyperglycemia, based on laboratory assessment of serum fasting glucose levels, occurred in 3.7% of patients. Two of 20 (10%) patients with diabetes or glucose intolerance at baseline required initiation of insulin while receiving ALUNBRIG.
Assess fasting serum glucose prior to initiation of ALUNBRIG and monitor periodically thereafter. Initiate or optimize antihyperglycemic medications as needed. If adequate hyperglycemic control cannot be achieved with optimal medical management, withhold ALUNBRIG until adequate hyperglycemic control is achieved and consider reducing the dose of ALUNBRIG as described in Table 1 or permanently discontinuing ALUNBRIG [see Dosage and Administration (2.2), Adverse Reactions (6.1)].
5.8 Embryo-Fetal Toxicity
Based on its mechanism of action and findings in animals, ALUNBRIG can cause fetal harm when administered to pregnant women. There are no clinical data on the use of ALUNBRIG in pregnant women. Administration of brigatinib to pregnant rats during the period of organogenesis resulted in dose-related skeletal anomalies at doses as low as 12.5 mg/kg/day (approximately 0.7 times the human exposure by AUC at 180 mg once daily), as well as increased post-implantation loss, malformations, and decreased fetal body weight at doses of 25 mg/kg/day (approximately 1.26 times the human exposure at 180 mg once daily) or higher.
Advise women of the potential risk to a fetus. Advise females of reproductive potential to use effective non-hormonal contraception during treatment with ALUNBRIG and for at least 4 months following the final dose. Advise males with female partners of reproductive potential to use effective contraception during treatment and for at least 3 months after the last dose of ALUNBRIG [see Use in Specific Populations (8.1, 8.3), Clinical Pharmacology (12.1)].
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the prescribing information:
Interstitial Lung Disease (ILD)/Pneumonitis [see Warnings and Precautions (5.1)]
Hypertension [see Warnings and Precautions (5.2)]
Bradycardia [see Warnings and Precautions (5.3)]
Visual Disturbance [see Warnings and Precautions (5.4)]
Creatine Phosphokinase (CPK) Elevation [see Warnings and Precautions (5.5)]
Pancreatic Enzymes Elevation [see Warnings and Precautions (5.6)]
Hyperglycemia [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of ALUNBRIG was evaluated in 219 patients with locally advanced or metastatic ALK-positive non-small cell lung cancer (NSCLC) who received at least 1 dose of ALUNBRIG in ALTA after experiencing disease progression on crizotinib. Patients received ALUNBRIG 90 mg once daily continuously (90 mg group) or 90 mg once daily for 7 days followed by 180 mg once daily (90→180 mg group). The median duration of treatment was 7.5 months in the 90 mg group and 7.8 months in the 90→180 mg group. A total of 150 (68%) patients were exposed to ALUNBRIG for greater than or equal to 6 months and 42 (19%) patients were exposed for greater than or equal to 1 year.
The study population characteristics were: median age 54 years (range: 18 to 82), age less than 65 years (77%), female (57%), White (67%), Asian (31%), Stage IV disease (98%), NSCLC adenocarcinoma histology (97%), never or former smoker (95%), ECOG Performance Status (PS) 0 or 1 (93%), and brain metastases at baseline (69%) [see Clinical Studies (14)].
Serious adverse reactions occurred in 38% of patients in the 90 mg group and 40% of patients in the 90→180 mg group. The most common serious adverse reactions were pneumonia (5.5% overall, 3.7% in the 90 mg group, and 7.3% in the 90→180 mg group) and ILD/pneumonitis (4.6% overall, 1.8% in the 90 mg group and 7.3% in the 90→180 mg group). Fatal adverse reactions occurred in 3.7% of patients and consisted of pneumonia (2 patients), sudden death, dyspnea, respiratory failure, pulmonary embolism, bacterial meningitis and urosepsis (1 patient each).
In ALTA, 2.8% of patients in the 90 mg group and 8.2% of patients in the 90→180 mg group permanently discontinued ALUNBRIG for adverse reactions. The most frequent adverse reactions that led to discontinuation were ILD/pneumonitis (0.9% in the 90 mg group and 1.8% in the 90→180 mg group) and pneumonia (1.8% in the 90→180 mg group only).
In ALTA, 14% of patients required a dose reduction due to adverse reactions (7.3% in the 90 mg group and 20% in the 90→180 mg group). The most common adverse reaction that led to dose reduction was increased creatine phosphokinase for both regimens (1.8% in the 90 mg group and 4.5% in the 90→180 mg group).
Table 3 and Table 4 summarize the common adverse reactions and laboratory abnormalities observed in ALTA.
Table 3: Adverse Reactions in ≥10% (All Grades*) or ≥2% (Grades 3-4) of Patients by Dose Group in ALTA (N=219)
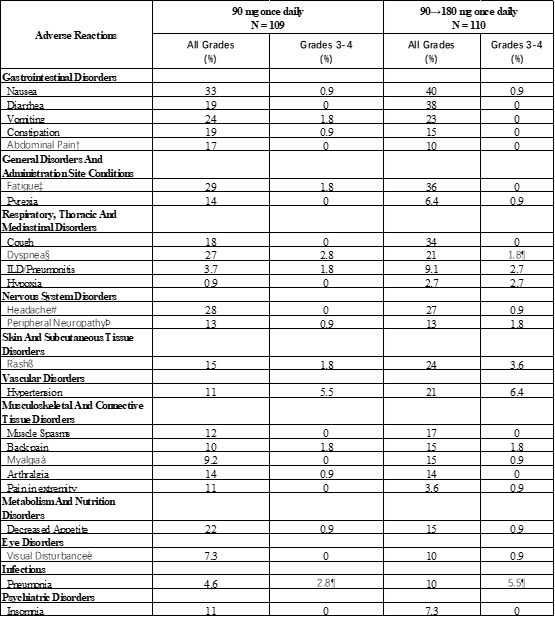
*Per National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 4.0
†Includes abdominal distension, abdominal pain, and epigastric discomfort
‡Includes asthenia and fatigue
§Includes dyspnea and exertional dyspnea
¶Includes one Grade 5 event
#Includes headache and sinus headache
ÞIncludes peripheral sensory neuropathy and paresthesia
ßIncludes acneiform dermatitis, exfoliative rash, rash, pruritic rash, and pustular rash
àIncludes musculoskeletal pain and myalgia
èIncludes diplopia, photophobia, blurred vision, reduced visual acuity, visual impairment, vitreous floaters, visual field defect, macular edema, and vitreous detachment
Table 4: Laboratory Abnormalities in ≥20% (All Grades*) of Patients by Regimen in ALTA (N=219)
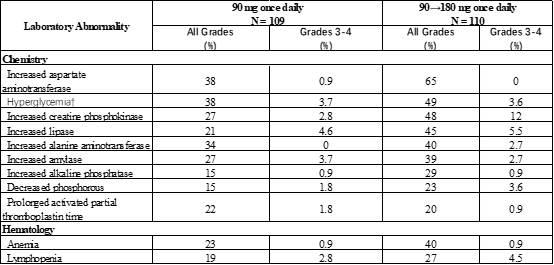
*Per CTCAE version 4.0
†Elevated blood insulin was also observed in both regimens
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on ALUNBRIG
Strong or Moderate CYP3A Inhibitors
Coadministration of ALUNBRIG with a strong or moderate CYP3A inhibitor increased brigatinib plasma concentrations, which may increase the incidence of adverse reactions [see Clinical Pharmacology (12.3)]. Avoid coadministration of ALUNBRIG with strong or moderate CYP3A inhibitors. If coadministration of strong or moderate CYP3A inhibitors cannot be avoided, modify dose as recommended [see Dosage and Administration (2.3)].
Strong or Moderate CYP3A Inducers
Coadministration of ALUNBRIG with a strong or moderate CYP3A inducer decreased brigatinib plasma concentrations, which may decrease the efficacy of ALUNBRIG [see Clinical Pharmacology (12.3)]. Avoid coadministration of ALUNBRIG with strong or moderate CYP3A inducers. If coadministration of moderate CYP3A inducers cannot be avoided, modify dose as recommended [see Dosage and Administration (2.4)].
7.2 Effect of ALUNBRIG on Other Drugs
CYP3A Substrates
Brigatinib may decrease the concentrations of sensitive CYP3A substrates. Coadministration of ALUNBRIG with CYP3A substrates, including hormonal contraceptives, can result in decreased concentrations and loss of efficacy of sensitive CYP3A substrates [see Use in Specific Populations (8.3)].
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on its mechanism of action and findings in animals, ALUNBRIG can cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. There are no clinical data on the use of ALUNBRIG in pregnant women. Administration of brigatinib to pregnant rats during the period of organogenesis resulted in dose-related skeletal anomalies at doses as low as 12.5 mg/kg/day (approximately 0.7 times the human exposure by AUC at 180 mg once daily) as well as increased post-implantation loss, malformations, and decreased fetal body weight at doses of 25 mg/kg/day (approximately 1.26 times the human exposure at 180 mg once daily) or greater (see Data). Advise pregnant women of the potential risk to a fetus.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In an embryo-fetal development study in which pregnant rats were administered daily doses of brigatinib during organogenesis, dose-related skeletal (incomplete ossification, small incisors) and visceral anomalies were observed at doses as low as 12.5 mg/kg/day (approximately 0.7 times the human exposure by AUC at 180 mg once daily). Malformations observed at 25 mg/kg/day (approximately 1.26 times the human AUC at 180 mg once daily) included anasarca (generalized subcutaneous edema), anophthalmia (absent eyes), forelimb hyperflexion, small, short and/or bent limbs, multiple fused ribs, bent scapulae, omphalocele (intestine protruding into umbilicus), and gastroschisis (intestines protruding through a defect in the abdominal wall) along with visceral findings of moderate bilateral dilatation of the lateral ventricles.
8.2 Lactation
Risk Summary
There are no data regarding the secretion of brigatinib in human milk or its effects on the breastfed infant or milk production. Because of the potential for adverse reactions in breastfed infants, advise lactating women not to breastfeed during treatment with ALUNBRIG and for 1 week following the final dose.
8.3 Females and Males of Reproductive Potential
Pregnancy Testing
Verify pregnancy status in females of reproductive potential prior to initiating ALUNBRIG [see Use in Specific Populations (8.1)].
Contraception
ALUNBRIG can cause fetal harm [see Use in Specific Populations (8.1)].
Females
Advise females of reproductive potential to use effective non-hormonal contraception during treatment with ALUNBRIG and for at least 4 months after the final dose. Counsel patients to use a non-hormonal method of contraception since ALUNBRIG can render some hormonal contraceptives ineffective [see Drug Interactions (7.2)].
Males
Because of the potential for genotoxicity, advise males with female partners of reproductive potential to use effective contraception during treatment with ALUNBRIG and for at least 3 months after the final dose [see Nonclinical Toxicology (13.1)].
Infertility
Based on findings in male reproductive organs in animals, ALUNBRIG may cause reduced fertility in males [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of ALUNBRIG in pediatric patients have not been established.
8.5 Geriatric Use
Clinical studies of ALUNBRIG did not include sufficient numbers of patients aged 65 years and older to determine whether they respond differently from younger patients.
8.6 Hepatic Impairment
No dose adjustment is recommended for patients with mild hepatic impairment (Child-Pugh A) or moderate hepatic impairment (Child-Pugh B). Reduce the dose of ALUNBRIG for patients with severe hepatic impairment (Child-Pugh C) [see Dosage and Administration (2.5), Clinical Pharmacology (12.3)].
8.7 Renal Impairment
No dose adjustment is recommended for patients with mild or moderate renal impairment [creatinine clearance (CLcr) 30 to 89 mL/min by Cockcroft-Gault]. Reduce the dose of ALUNBRIG for patients with severe renal impairment (CLcr 15 to 29 mL/min) [see Dosage and Administration (2.6), Clinical Pharmacology (12.3)].
11 DESCRIPTION
Brigatinib is a kinase inhibitor. The chemical name for brigatinib is 5-chloro-N4-[2-(dimethylphosphoryl)phenyl]-N2-{2-methoxy-4-[4-(4-methylpiperazin-1-yl)piperidin-1-yl]phenyl}pyrimidine-2,4-diamine. The molecular formula is C29H39ClN7O2P which corresponds to a formula weight of 584.10 g/mol. Brigatinib has no chiral centers. The chemical structure is shown below:
Brigatinib is an off-white to beige/tan solid. The pKas were determined to be: 1.73 ± 0.02 (base), 3.65 ± 0.01 (base), 4.72 ± 0.01 (base), and 8.04 ± 0.01 (base).
ALUNBRIG is supplied for oral use as film-coated tablets containing 180 mg, 90 mg or 30 mg of brigatinib and the following inactive ingredients: lactose monohydrate, microcrystalline cellulose, sodium starch glycolate (Type A), magnesium stearate, and hydrophobic colloidal silica. The tablet coating consists of talc, polyethylene glycol, polyvinyl alcohol, and titanium dioxide.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Brigatinib is a tyrosine kinase inhibitor with in vitro activity at clinically achievable concentrations against multiple kinases including ALK, ROS1, insulin-like growth factor-1 receptor (IGF-1R), and FLT-3 as well as EGFR deletion and point mutations. Brigatinib inhibited autophosphorylation of ALK and ALK-mediated phosphorylation of the downstream signaling proteins STAT3, AKT, ERK1/2, and S6 in in vitro and in vivo assays. Brigatinib also inhibited the in vitro proliferation of cell lines expressing EML4-ALK and NPM-ALK fusion proteins and demonstrated dose-dependent inhibition of EML4-ALK-positive NSCLC xenograft growth in mice.
At clinically achievable concentrations (≤500 nM), brigatinib inhibited the in vitro viability of cells expressing EML4-ALK and 17 mutant forms associated with resistance to ALK inhibitors including crizotinib, as well as EGFR-Del (E746-A750), ROS1-L2026M, FLT3-F691L, and FLT3-D835Y. Brigatinib exhibited in vivo antitumor activity against 4 mutant forms of EML4-ALK, including G1202R and L1196M mutants identified in NSCLC tumors in patients who have progressed on crizotinib. Brigatinib also reduced tumor burden and prolonged survival in mice implanted intracranially with an ALK-driven tumor cell line.
12.2 Pharmacodynamics
Brigatinib exposure-response relationships and the time course of the pharmacodynamic response are unknown.
Cardiac Electrophysiology
The QT interval prolongation potential of ALUNBRIG was assessed in 123 patients following once daily ALUNBRIG doses of 30 mg (0.16 times the recommended dose of 180 mg) to 240 mg (1.3 times the recommended dose of 180 mg). ALUNBRIG did not prolong the QT interval to a clinically relevant extent.
12.3 Pharmacokinetics
The geometric mean (CV%) steady-state maximum concentration (Cmax) of brigatinib at ALUNBRIG doses of 90 mg and 180 mg once daily was 552 (65%) ng/mL and 1452 (60%) ng/mL, respectively, and the corresponding area under the concentration-time curve (AUC0-Tau) was 8165 (57%) ng∙h/mL and 20276 (56%) ng∙h/mL. After a single dose and multiple dosing of ALUNBRIG, systemic exposure of brigatinib was dose proportional over the dose range of 60 mg (0.3 times the recommended dose of 180 mg) to 240 mg (1.3 times the recommended dose of 180 mg) once daily. The mean accumulation ratio after repeat dosing was 1.9 to 2.4.
Absorption
Following administration of single oral doses of ALUNBRIG of 30 mg to 240 mg, the median time to peak concentration (Tmax) ranged from 1 to 4 hours.
Effect of Food
Brigatinib Cmax was reduced by 13% with no effect on AUC in healthy subjects administered ALUNBRIG after a high fat meal (approximately 920 calories, 58 grams carbohydrate, 59 grams fat and 40 grams protein) compared to the Cmax and AUC after overnight fasting.
Distribution
Brigatinib is 91% bound to human plasma proteins and the binding is not concentration-dependent. The blood-to-plasma concentration ratio is 0.69. Following oral administration of ALUNBRIG 180 mg once daily, the mean apparent volume of distribution (Vz/F) of brigatinib at steady-state was 153 L.
Elimination
Following oral administration of ALUNBRIG 180 mg once daily, the mean apparent oral clearance (CL/F) of brigatinib at steady-state is 12.7 L/h and the mean plasma elimination half-life is 25 hours.
Metabolism
Brigatinib is primarily metabolized by CYP2C8 and CYP3A4 in vitro. Following oral administration of a single 180 mg dose of radiolabeled brigatinib to healthy subjects, N-demethylation and cysteine conjugation were the two major metabolic pathways. Unchanged brigatinib (92%) was the major circulating radioactive component.
Excretion
Following oral administration of a single 180 mg dose of radiolabeled brigatinib to healthy subjects, 65% of the administered dose was recovered in feces and 25% of the administered dose was recovered in urine. Unchanged brigatinib represented 41% and 86% of the total radioactivity in feces and urine, respectively.
Specific Populations
Age, race, sex, body weight, and albumin concentration have no clinically meaningful effect on the pharmacokinetics of brigatinib.
Patients with Hepatic Impairment
Following a single dose of ALUNBRIG 90 mg, unbound brigatinib systemic exposure (AUC0-INF) was 37% higher in subjects with severe hepatic impairment (Child-Pugh C) compared to subjects with normal hepatic function. Unbound brigatinib systemic exposure (AUC0-INF) was similar between subjects with mild (Child-Pugh A) to moderate (Child-Pugh B) hepatic impairment and subjects with normal hepatic function [see Dosage and Administration (2.5)].
Patients with Renal Impairment
Following a single dose of ALUNBRIG 90 mg, unbound brigatinib systemic exposure (AUC0-INF) was 86% higher in subjects with severe renal impairment [creatinine clearance (CLcr) 15 to 29 mL/min] compared to subjects with normal renal function.
Based on a population pharmacokinetic analysis, brigatinib exposures were similar among 125 subjects with mild renal impairment (CLcr 60 to 89 mL/min), 34 subjects with moderate renal impairment (CLcr 30 to 59 mL/min) and 270 subjects with normal renal function (CLcr ≥90 mL/min) [see Dosage and Administration (2.6)].
Drug Interaction Studies
Clinical Studies
Effect of Strong and Moderate CYP3A Inhibitors on Brigatinib:
Coadministration of 200 mg twice daily doses of itraconazole (a strong CYP3A inhibitor) with a single 90 mg dose of ALUNBRIG increased brigatinib Cmax by 21% and AUC0-INF by 101%, relative to a 90 mg dose of ALUNBRIG administered alone [see Dosage and Administration (2.3), Drug Interactions (7.1)]. A moderate CYP3A inhibitor is predicted to increase the AUC of brigatinib by approximately 40%.
Effect of Strong CYP2C8 Inhibitors on Brigatinib:
Coadministration of 600 mg twice daily doses of gemfibrozil (a strong CYP2C8 inhibitor) with a single 90 mg dose of ALUNBRIG decreased brigatinib Cmax by 41% and AUC0-INF by 12%, relative to a 90 mg dose of ALUNBRIG administered alone. The effect of gemfibrozil on the pharmacokinetics of brigatinib is not clinically meaningful and the underlying mechanism for the decreased exposure of brigatinib is unknown.
Effect of Strong and Moderate CYP3A Inducers on Brigatinib:
Coadministration of 600 mg daily doses of rifampin (a strong CYP3A inducer) with a single 180 mg dose of ALUNBRIG decreased brigatinib Cmax by 60% and AUC0-INF by 80%, relative to a 180 mg dose of ALUNBRIG administered alone [see Dosage and Administration (2.4), Drug Interactions (7.1)]. A moderate CYP3A inducer is predicted to decrease the AUC of brigatinib by approximately 50%.
In Vitro Studies
Effect of Brigatinib on CYP Enzymes:
Brigatinib, at clinically relevant plasma concentrations, induced CYP3A via activation of the pregnane X receptor (PXR). Brigatinib may also induce CYP2C enzymes via the same mechanism at clinically relevant concentrations.
Brigatinib did not inhibit CYP1A2, 2B6, 2C8, 2C9, 2C19, 2D6, or 3A4/5 at clinically relevant concentrations.
Effect of P-glycoprotein and BCRP Inhibitors on Brigatinib:
Brigatinib is a substrate of the efflux transporters P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP). Given that brigatinib exhibits high solubility and high permeability in vitro, P-gp and BCRP inhibitors are unlikely to increase plasma concentrations of brigatinib.
Effect of Other Transporters on Brigatinib:
Brigatinib is not a substrate of organic anion transporting polypeptide (OATP1B1, OATP1B3), organic anion transporter (OAT1, OAT3), organic cation transporter (OCT1, OCT2), multidrug and toxin extrusion protein (MATE1, MATE2K), or bile salt export pump (BSEP).
Effect of Brigatinib on Transporters:
Brigatinib is an inhibitor of P-gp, BCRP, OCT1, MATE1, and MATE2K in vitro. Therefore, brigatinib may have the potential to increase concentrations of coadministered substrates of these transporters. Brigatinib at clinically relevant concentrations did not inhibit OATP1B1, OATP1B3, OAT1, OAT3, OCT2 or BSEP.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been performed with brigatinib.
Treatment with brigatinib resulted in chromosomal damage in an in vivo mammalian erythrocyte micronucleus in the rat, but was not mutagenic in the Ames or in vitro mammalian chromosome aberration tests.
Dedicated animal fertility studies were not conducted with brigatinib. Testicular toxicity was observed in repeat-dose animal studies at doses resulting in exposure as low as 0.2 times the exposure in patients at the 180 mg dose. In rats, findings included lower weight of testes, seminal vesicles and prostate gland, and testicular tubular degeneration; these effects were not reversible during the 2 month recovery period. In monkeys, findings included reduced size of testes along with microscopic evidence of hypospermatogenesis; these effects were reversible during the recovery period.
14 CLINICAL STUDIES
The efficacy of ALUNBRIG was demonstrated in a two-arm, open-label, multicenter trial (ALTA, NCT02094573) in adult patients with locally advanced or metastatic ALK-positive non-small cell lung cancer (NSCLC) who had progressed on crizotinib. The study required patients to have a documented ALK rearrangement based on an FDA-approved test or a different test with adequate archival tissue to confirm ALK arrangement by the Vysis® ALK Break-Apart fluorescence in situ hybridization (FISH) Probe Kit test. Key eligibility criteria included an ECOG Performance Status of 0-2 and progression on crizotinib. Neurologically stable patients with central nervous system (CNS) metastases were permitted to enroll. Patients with a history of interstitial lung disease or drug-related pneumonitis or who had received crizotinib within 3 days of the first dose of brigatinib were excluded. The major efficacy outcome measure was confirmed overall response rate (ORR) according to Response Evaluation Criteria in Solid Tumors (RECIST v1.1) as evaluated by an Independent Review Committee (IRC). Additional efficacy outcome measures included Investigator-assessed ORR, duration of response (DOR), intracranial ORR, and intracranial DOR.
A total of 222 patients were randomized to receive ALUNBRIG either 90 mg once daily (90 mg arm; n=112) or 180 mg once daily following a 7-day lead-in at 90 mg once daily (90→180 mg arm; n=110). Randomization was stratified by brain metastases (present vs absent) and best prior response to crizotinib (complete or partial response vs any other response/unevaluable).
Baseline demographic characteristics of the overall study population were: median age 54 years (range 18 to 82, 23% 65 and over), 67% White and 31% Asian, 57% female, 36% ECOG PS 0 and 57% ECOG PS 1, and 95% never or former smokers. The disease characteristics of the overall study population were: Stage IV disease in 98%, adenocarcinoma histology in 97%, prior systemic chemotherapy in 74%, metastatic disease to the brain in 69% (61% had received prior radiation to the brain), bone metastases in 39%, and liver metastases in 26% of patients. Sixty-four percent of patients had an objective response to prior crizotinib.
The median duration of follow-up was 8 months (range: 0.1-20.2). Efficacy results from ALTA are summarized in Table 5.
Table 5: ALTA Efficacy Results
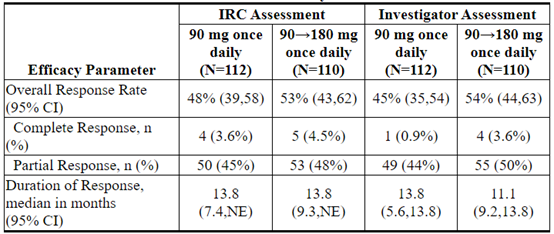
CI = Confidence Interval; NE = Not Estimable
IRC assessment of intracranial ORR and intracranial DOR according to RECIST v1.1 in the subgroup of 44 patients with measurable brain metastases (≥10 mm in longest diameter) at baseline are summarized in Table 6. Duration of intracranial response was measured from date of first intracranial response until intracranial disease progression (new lesions, intracranial target lesion diameter growth ≥20% from nadir, or unequivocal progression of intracranial nontarget lesions) or death.
Table 6: Intracranial Overall Response in Patients with Measurable Brain Metastases in ALTA
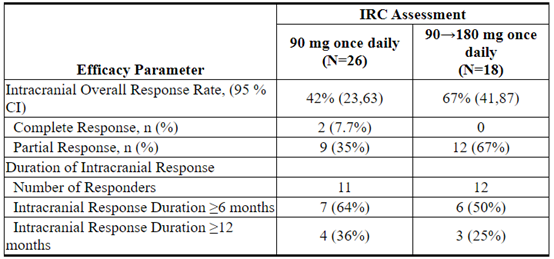
CI = Confidence Interval
16 HOW SUPPLIED/STORAGE AND HANDLING
180 mg tablets: oval, white to off-white film-coated tablets with "U13" debossed on one side and plain on the other side; available in:

90 mg tablets: oval, white to off-white film-coated tablets with "U7" debossed on one side and plain on the other side; available in:

30 mg tablets: round, white to off-white film-coated tablets with "U3" debossed on one side and plain on the other side; available in:

90 mg / 7 count tablets (NDC 63020-090-07) and 180 mg / 23 count tablets (NDC 63020-180-23) are also available in a single carton as a one-month initiation pack:
Store at controlled room temperature 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) (see USP).
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Interstitial Lung Disease (ILD)/Pneumonitis
Inform patients of the symptoms and risks of serious pulmonary adverse reactions such as ILD/pneumonitis. Advise patients to immediately report any new or worsening respiratory symptoms [see Warnings and Precautions (5.1)].
Hypertension
Advise patients of risks of hypertension and to promptly report signs or symptoms of hypertension [see Warnings and Precautions (5.2)].
Bradycardia
Advise patients to report any symptoms of bradycardia and to inform their healthcare provider about the use of heart and blood pressure medications [see Warnings and Precautions (5.3)].
Visual Disturbance
Advise patients to inform their healthcare provider of any new or worsening vision symptoms [see Warnings and Precautions (5.4)].
Creatine Phosphokinase (CPK) Elevation
Inform patients of the signs and symptoms of creatinine phosphokinase (CPK) elevation and the need for monitoring during treatment. Advise patients to inform their healthcare provider of any new or worsening symptoms of unexplained muscle pain, tenderness, or weakness [see Warnings and Precautions (5.5)].
Pancreatic Enzymes Elevation
Inform patients of the signs and symptoms of pancreatitis and the need to monitor for amylase and lipase elevations during treatment [see Warnings and Precautions (5.6)].
Hyperglycemia
Inform patients of the risks of new or worsening hyperglycemia and the need to periodically monitor glucose levels. Advise patients with diabetes mellitus or glucose intolerance that antihyperglycemic medications may need to be adjusted during treatment with ALUNBRIG [see Warnings and Precautions (5.7)].
Females and Males of Reproductive Potential
Embryo-Fetal Toxicity
Advise females and males of reproductive potential that ALUNBRIG can cause fetal harm [see Warnings and Precautions (5.8), Use in Specific Populations (8.1)].
Advise females of reproductive potential to inform their healthcare provider of a known or suspected pregnancy and to use effective non-hormonal contraception during treatment with ALUNBRIG and for at least 4 months after the final dose [see Use in Specific Populations (8.3)].
Advise males with female partners of reproductive potential to use effective contraception during treatment with ALUNBRIG and for at least 3 months after the final dose [see Use in Specific Populations (8.3)].
Lactation
Advise females not to breastfeed during treatment with ALUNBRIG and for at least 1 week following the final dose [see Use in Specific Populations (8.2)].
Infertility
Advise males of reproductive potential of the potential for reduced fertility from ALUNBRIG [see Use in Specific Populations (8.3), Nonclinical Toxicology (13.1)].
Drug Interactions
Advise patients to inform their healthcare provider of all concomitant medications, including prescription medicines, over-the-counter drugs, vitamins, and herbal products. Inform patients to avoid grapefruit or grapefruit juice while taking ALUNBRIG [see Drug Interactions (7)].
Dosing and Administration
Instruct patients to start with 90 mg of ALUNBRIG once daily for the first 7 days and if tolerated, increase the dose to 180 mg once daily. Advise patients to take ALUNBRIG with or without food [see Dosage and Administration (2.1)].
Missed Dose
Advise patients that if a dose of ALUNBRIG is missed or if the patient vomits after taking a dose of ALUNBRIG, not to take an extra dose, but to take the next dose at the regular time [see Dosage and Administration (2.1)].
Manufactured for:
Takeda Pharmaceutical Company Limited
40 Landsdowne Street, Cambridge, MA 02139-4234
ALUNBRIG® is a registered trademark of ARIAD Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.
©2017-2018 ARIAD Pharmaceuticals, Inc. All rights reserved.
ABG346 R2
PATIENT INFORMATION
ALUNBRIG (uh-lun-brig)
(brigatinib)
tabletsWhat is the most important information I should know about ALUNBRIG?
ALUNBRIG can cause serious side effects, including:- Lung problems. ALUNBRIG may cause severe or life-threatening swelling (inflammation) of the lungs any time during treatment, and can lead to death. These lung problems happen especially within the first week of treatment with ALUNBRIG. Symptoms may be similar to those symptoms from lung cancer. Tell your healthcare provider right away if you have any new or worsening symptoms, including:
- trouble breathing or shortness of breath
- chest pain
- cough with or without mucus
- fever
- High blood pressure (hypertension). ALUNBRIG may cause high blood pressure. Your healthcare provider will check your blood pressure before starting and during treatment with ALUNBRIG. Tell your healthcare provider right away if you get headaches, dizziness, blurred vision, chest pain or shortness of breath.
- Slow heart rate (bradycardia). ALUNBRIG may cause very slow heartbeats that can be severe. Your healthcare provider will check your heart rate during treatment with ALUNBRIG. Tell your healthcare provider right away if you feel dizzy, lightheaded, or faint during treatment with ALUNBRIG. Tell your healthcare provider if you start to take or have any changes in heart or blood pressure medicines.
- Vision problems. ALUNBRIG may cause vision problems. Your healthcare provider may stop ALUNBRIG and refer you to an eye specialist if you develop severe vision problems during treatment with ALUNBRIG. Tell your healthcare provider right away if you have any loss of vision or any change in vision, including:
- double vision
- seeing flashes of light
- blurry vision
- light hurting your eyes
- new or increased floaters
- Muscle pain, tenderness, and weakness (myalgia). ALUNBRIG may increase the level of an enzyme in your blood called creatine phosphokinase (CPK), which may be a sign of muscle damage. Your healthcare provider will do blood tests to check your blood levels of CPK during treatment with ALUNBRIG. Tell your healthcare provider right away if you get new or worsening signs and symptoms of muscle problems, including unexplained muscle pain or muscle pain that does not go away, tenderness, or weakness.
- Inflammation of the pancreas (pancreatitis). ALUNBRIG may increase enzymes in your blood called amylase and lipase, which may be a sign of pancreatitis. Your healthcare provider will do blood tests to check your pancreatic enzyme blood levels during treatment with ALUNBRIG. Tell your healthcare provider right away if you get new or worsening signs and symptoms of pancreatitis, including upper abdominal pain that may spread to the back and get worse with eating, weight loss, or nausea.
- High blood sugar (hyperglycemia). ALUNBRIG may increase your blood sugar levels. Your healthcare provider will do blood tests to check your blood sugar levels before starting and during treatment with ALUNBRIG. Your healthcare provider may need to start or change your blood sugar medicine to control your blood sugar levels. Tell your healthcare provider right away if you get new or worsening signs and symptoms of hyperglycemia, including:
- feeling very thirsty
- needing to urinate more than usual
- feeling very hungry
- feeling sick to your stomach
- feeling weak or tired
- feeling confused
See "What are the possible side effects of ALUNBRIG?" for information about side effects. What is ALUNBRIG?
ALUNBRIG is a prescription medicine used to treat people with non-small cell lung cancer (NSCLC):- that has a certain type of abnormal anaplastic lymphoma kinase (ALK) gene, and
- that has spread to other parts of your body, and
- who have taken the medicine crizotinib, but their NSCLC worsened or they cannot tolerate taking crizotinib.
It is not known if ALUNBRIG is safe and effective in children.
Before you take ALUNBRIG, tell your healthcare provider about all of your medical conditions, including if you:
- have lung or breathing problems
- have high blood pressure
- have a slow heartbeat
- have any vision problems
- have or have had pancreatitis
- have diabetes mellitus or glucose intolerance
- have liver problems
- have kidney problems or are on dialysis
- are pregnant or plan to become pregnant. ALUNBRIG can harm your unborn baby. Your healthcare provider will determine whether or not you are pregnant before you start treatment with ALUNBRIG. Tell your healthcare provider right away if you become pregnant during treatment with ALUNBRIG or think you may be pregnant.
- Females who are able to become pregnant should use effective non-hormonal birth control during treatment with ALUNBRIG and for at least 4 months after the final dose of ALUNBRIG. Birth control pills (oral contraceptives) and other hormonal forms of birth control may not be effective if used during treatment with ALUNBRIG. Talk to your healthcare provider about birth control choices that are right for you during treatment with ALUNBRIG.
- Males who have female partners that are able to become pregnant should use effective birth control during treatment with ALUNBRIG and for at least 3 months after the final dose of ALUNBRIG.
- are breastfeeding or plan to breastfeed. It is not known if ALUNBRIG passes into your breast milk. Do not breastfeed during treatment with ALUNBRIG and for 1 week after the final dose of ALUNBRIG.
Tell your healthcare provider about all the medicines you take, including prescription medicines, over-the-counter medicines, vitamins, or herbal supplements.
How should I take ALUNBRIG?
- Take ALUNBRIG exactly as your healthcare provider tells you to take it. Do not change your dose or stop taking ALUNBRIG unless your healthcare provider tells you to.
- Your healthcare provider will start you on a low dose (90 mg) of ALUNBRIG for the first 7 days of treatment. If you tolerate this dose of ALUNBRIG well, your healthcare provider may increase your dose after the first 7 days of treatment.
- Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with ALUNBRIG if you develop side effects.
- Take ALUNBRIG 1 time each day.
- Take ALUNBRIG with or without food.
- Swallow ALUNBRIG tablets whole. Do not crush or chew tablets.
- If you miss a dose of ALUNBRIG, do not take the missed dose. Take your next dose at your regular time.
- If you vomit after taking a dose of ALUNBRIG, do not take an extra dose. Take your next dose at your regular time.
What should I avoid while taking ALUNBRIG?
- Avoid eating grapefruit or drinking grapefruit juice during treatment with ALUNBRIG. Grapefruit may increase the amount of ALUNBRIG in your blood.
What are the possible side effects of ALUNBRIG?
ALUNBRIG may cause serious side effects, including:The most common side effects of ALUNBRIG include:
- nausea
- diarrhea
- fatigue
- cough
- headache
ALUNBRIG may cause fertility problems in males. This may affect your ability to father a child. Talk to your healthcare provider if you have concerns about fertility.
These are not all of the possible side effects of ALUNBRIG.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How should I store ALUNBRIG?
- Store ALUNBRIG at room temperature 20°C to 25°C (68°F to 77°F).
Keep ALUNBRIG and all medicines out of the reach of children.
General information about the safe and effective use of ALUNBRIG.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use ALUNBRIG for a condition for which it was not prescribed. Do not give ALUNBRIG to other people, even if they have the same symptoms you have. It may harm them.
You can ask your healthcare provider or pharmacist for information about ALUNBRIG that is written for health professionals.What are the ingredients in ALUNBRIG?
Active ingredient: brigatinib
Inactive ingredients: lactose monohydrate, microcrystalline cellulose, sodium starch glycolate (Type A), magnesium stearate, and hydrophobic colloidal silica. The tablet coating consists of talc, polyethylene glycol, polyvinyl alcohol, and titanium dioxide.
Manufactured for: Takeda Pharmaceutical Company Limited, 40 Landsdowne Street, Cambridge, MA 02139-4234. ALUNBRIG® is a registered trademark of ARIAD Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited. ©2017-2018 ARIAD Pharmaceuticals, Inc. All rights reserved.
For more information, go to www.alunbrig.com or call 1-844-A-1POINT (1-844-217-6468).This Patient Information has been approved by the U.S. Food and Drug Administration ABG346 R2 Revised: December 2018
PRINCIPAL DISPLAY PANEL - 30 mg Tablet Bottle Carton
NDC 63020-113-30
ALUNBRIG™
(brigatinib) tablets30 mg
Rx Only
30 Tablets
PRINCIPAL DISPLAY PANEL - 90 mg Tablet Bottle Carton
NDC 63020-090-30
ALUNBRIG™
(brigatinib) tablets90 mg
Rx Only
30 Tablets
PRINCIPAL DISPLAY PANEL - 180 mg Tablet Bottle Carton
NDC 63020-180-30
ALUNBRIG™
(brigatinib) tablets180 mg
Rx Only
30 Tablets
PRINCIPAL DISPLAY PANEL - Kit Carton
NDC 63020-198-30
INITIATION PACKALUNBRIG™
(brigatinib) tabletsRx Only | Oral Use
Usual Dose: One 90 mg tablet orally once daily for the first 7 days;
if tolerated, increase to one 180 mg tablet orally once daily.
See accompanying full Prescribing Information for complete details.90 mg
7 Tablets
Take 1 tablet on
Day 1 - Day 7180 mg
23 Tablets
Take 1 tablet on
Day 8 - Day 30
【备注】以上内容仅供参考,不作为用药依据,详情请参照药品附带说明书。
本说明书来源于美国FDA
https://nctr-crs.fda.gov/fdalabel/services/spl/set-ids/0fe9ff20-d402-41f3-bc1e-7002ea7007db/spl-doc?hl=ALUNBRIG
-
-
-

-
通用名: 塞瑞替尼胶囊
商品名: Cerinib
规格: 150mg×30粒
产地: 孟加拉国药二厂(Drug International Ltd. Unit-2)
国际参考零售价:¥**/盒
-
-
-

-
-
-
-
-
通用名: 布格替尼片
商品名: LuciBriga 90
规格: 90mg×30片
产地: 卢修斯医药(老挝)有限公司(LUCIUS PHARMACEUTICALS(LAO) CO.,LTD)
国际参考零售价:¥**/盒
-

通用名: 洛拉替尼片
商品名: Lorbrexen
规格: 100mg×30片
产地: 孟加拉珠峰制药(Everest Pharmaceuticals Ltd.)
国际参考零售价:¥**/盒
-